Introduction
Patients in the intensive care unit (ICU) differ from those on the general ward since they are often sedated for mechanical ventilation [1] or have an altered mental status. Subsequently, several aspects of care are more vulnerable to neglect, particularly oral care. Serious failings exist in the assessment of oral health and its risk factors in the ICU [2]. Checking the number of teeth and the condition they are in is crucial in ICU patient care but is often neglected.
A dental bridge is a prosthesis consisting of 2 crowns and 1 or more artificial teeth that is used to fill the hole created by a missing tooth. A bridge is inserted using the natural teeth as pillars next to the hole. Bridges can be made from metal, ceramic, or a combination of both [1].
Here we introduce 3 cases in which the loss of a dental bridge was missed by the ICU staff, and discuss potential complications, and suggest possible solutions to reduce future incidences of dental bridge loss.
Case Report
1. Case 1
A 79-year-old man (172 cm, 68 kg) was admitted due to suspected enteritis and sepsis. On the 3rd day of hospital admission (HOD 3), he was transferred to the ICU with septic shock. The nurse’s medical record, listed his oral health as very poor prior to ICU admission. On HOD 8, abdominal computed tomography revealed multiple small bowel perforations and a gangrenous gallbladder. Consequently, emergency surgery with small bowel segmental resection and cholecystectomy was performed. Following surgery, he returned to the ICU for management along with mechanical ventilator support with an endotracheal tube inserted by an anesthesiologist in the operating room.
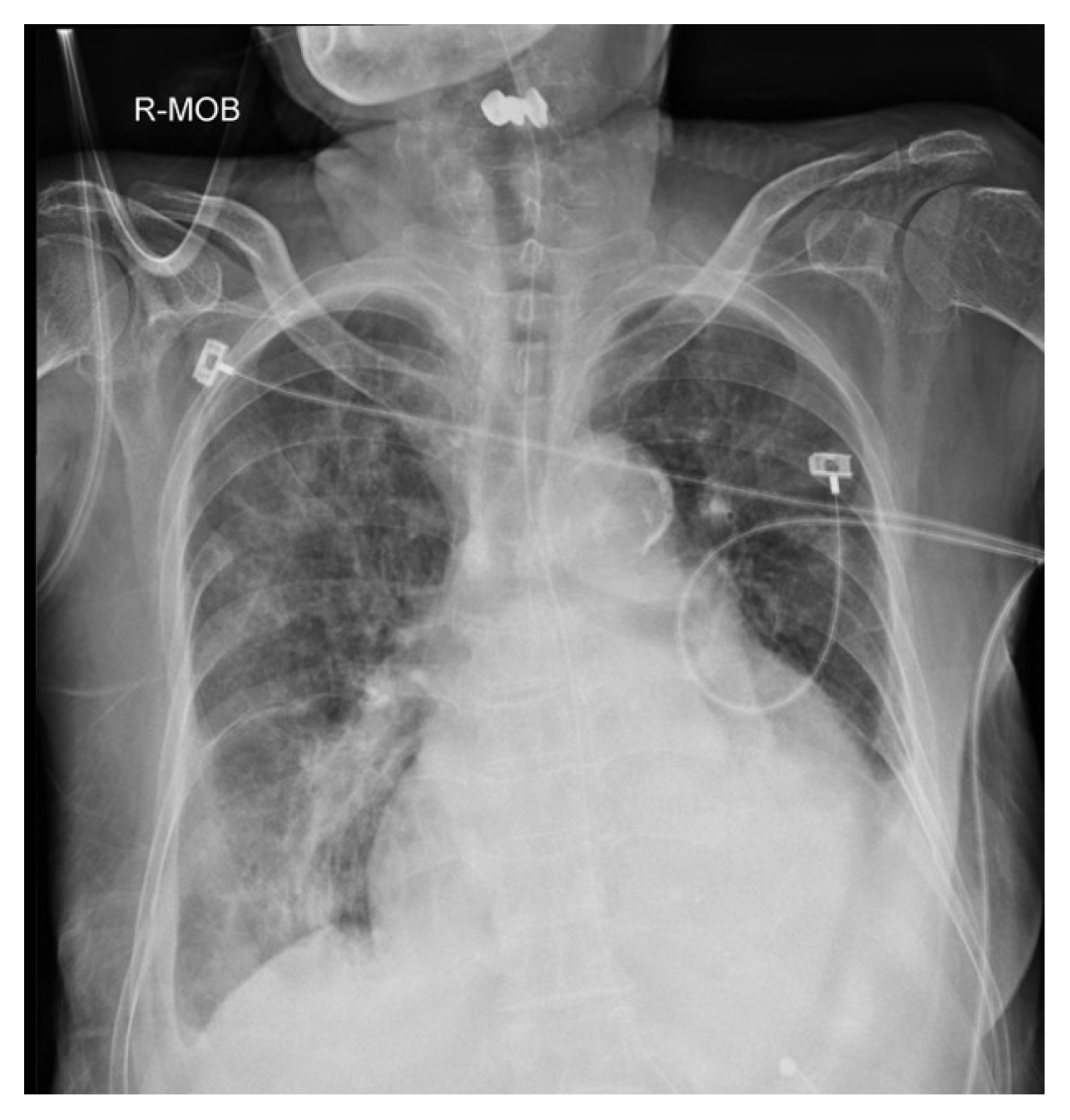
On the 16th postoperative day (POD 16), a dental bridge was observed in the pharynx on a daily routine chest X-ray image (Figure 1). A retrospective review revealed that this dental bridge had been missing since POD 12. All physicians and nurses had failed to recognize its absence. The dental bridge located in the pharynx was removed by a surgical intensivist under video laryngoscopy guidance.
2. Case 2
A 79-year-old female patient (155 cm, 49 kg) was admitted to the ICU after undergoing a Hartmann’s operation for rectal cancer. She was transferred to the ICU postoperatively due to a cardiac arrest of respiratory origin that occurred in the recovery room. She was emergently intubated in the postoperative recovery room by an anesthesiologist. Recovery of spontaneous circulation was achieved following immediate intubation and 6 minutes of cardiac compression. Weaning from mechanical ventilation was successfully achieved on POD 5. However, her mental status indicated mild drowsiness, and she could not expectorate very well. She required several days of further observation in the ICU. Her oral condition was poor and she had lost many teeth.
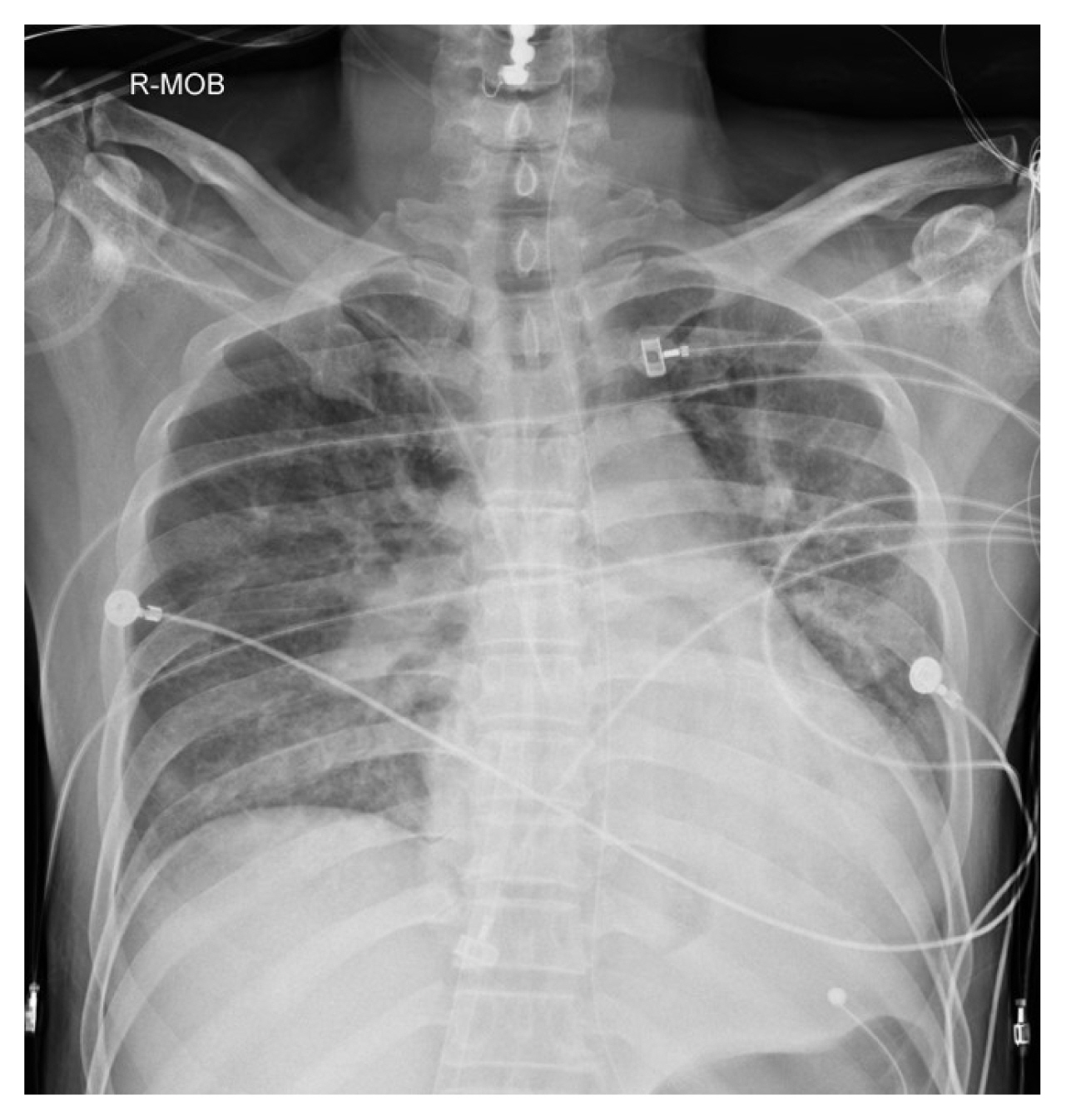
On POD 13, a dental bridge was observed in the throat area on a daily routine chest X-ray image (Figure 2). A retrospective review of the patient’s chart revealed that this dental bridge should have been recognized as missing on POD 8 but it had been overlooked by all physicians and nurses involved in the patient’s care. The dental bridge was successfully removed using a long Kelly under video laryngoscopy guidance whilst the patient was mildly sedated.
3. Case 3
A 51-year-old man (177cm, 72kg) who received cardiopulmonary resuscitation due to ventricular fibrillation with cardiogenic shock was transferred to the ER. An emergency doctor immediately intubated him and inserted a venoarterial cannula for extracorporeal membrane oxygenation (ECMO). This was followed by a coronary angiography which showed a proximal left anterior descending artery thrombosis, so a stent was inserted.
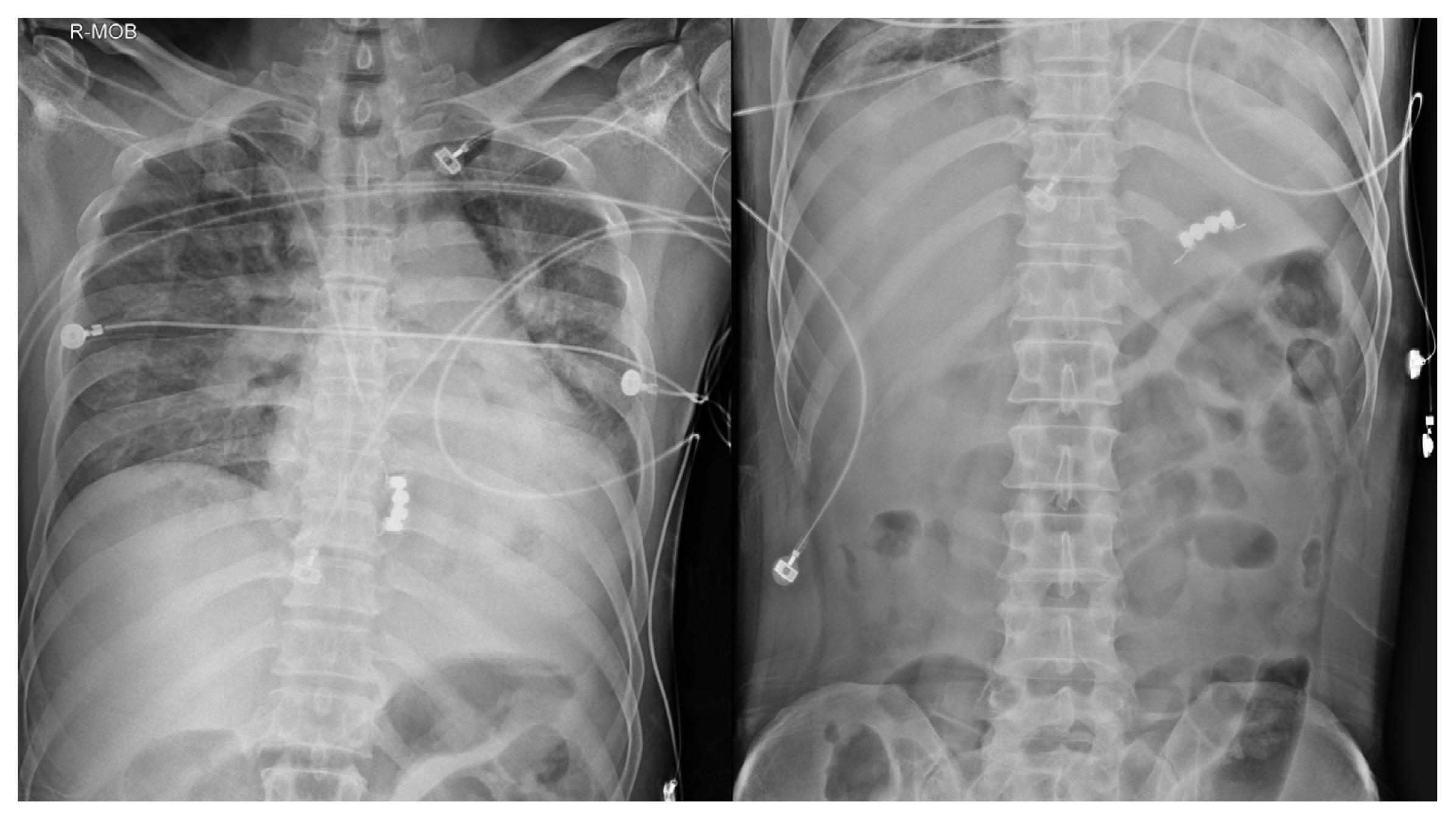
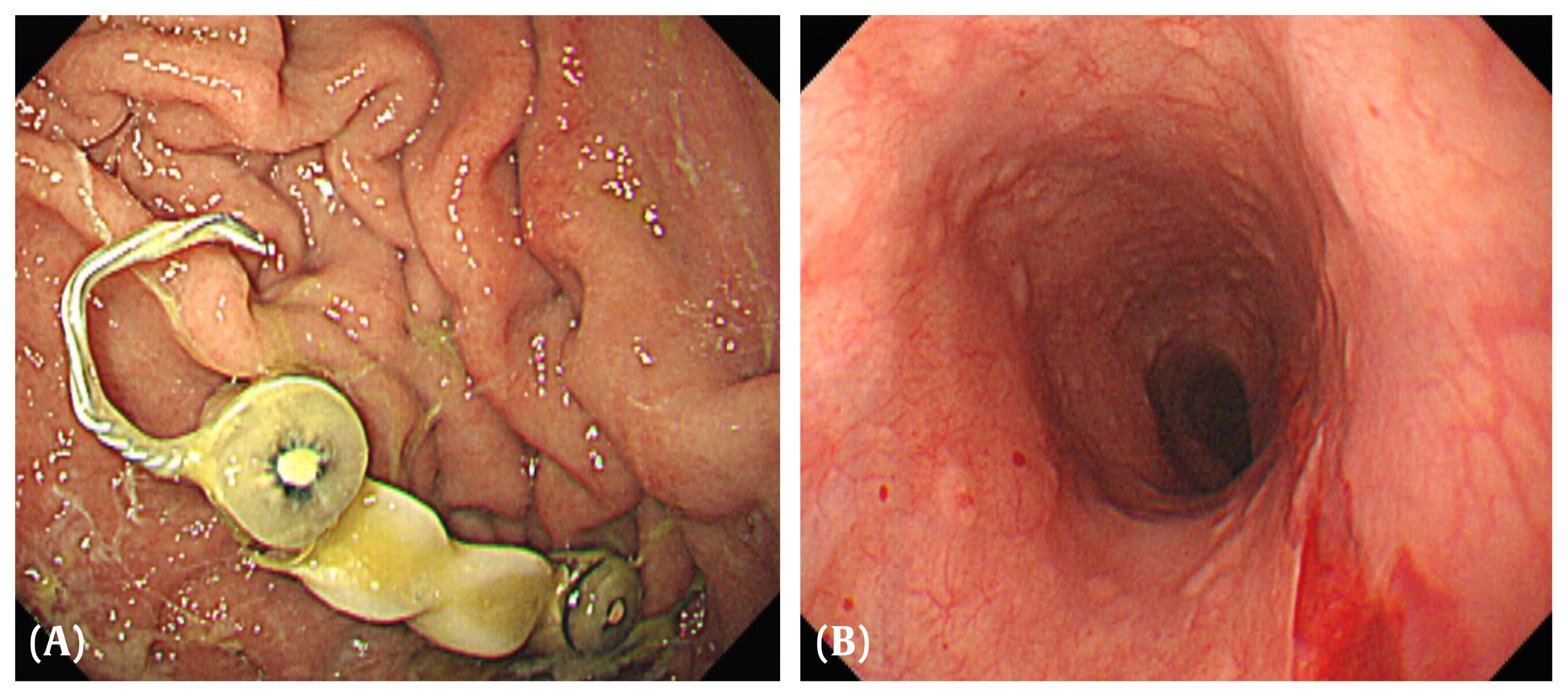
He was extubated on HOD 2. His oral condition was not poor. The patient showed dysphagia as dietary advancement progressed, but it was considered clinically insignificant. On HOD 3, the ECMO was removed. At this time, a dental bridge was observed in the hypopharynx area on the previous day’s chest X-ray image (Figure 3). A follow-up chest X-ray revealed that the dental bridge was now in the stomach (Figure 4). On HOD 4, he underwent endoscopic foreign body removal (Figure 5). On HOD 15, a follow-up endoscopy revealed signs of healing. He was discharged on HOD 20.
This study was approved by the Korea University Anam Hospital Institutional Review Board (IRB approval number 2020AN0192). Prior consent was not required for this study.
Discussion
Tooth loss and tooth aspiration is a critical problem that can have life-threatening complications [4]. Zhang et al [5] presented 3 cases of tooth aspiration following multiple trauma in which the need for tooth aspiration was missed by local hospitals. The authors emphasized the importance of suspecting the need for aspiration in cases of dental avulsion, especially in comatose patients.
Multiple cases have also been reported of tooth loss and tooth aspiration following endotracheal intubation [6–8]. The incidence of dental injury following endotracheal intubation is reportedly 0.17–12.1% [6]. Alabidi [7] reported a case of aspiration of an incisor tooth post-adenotonsillectomy in a 10-year-old boy. The author provided several recommendations prior to intubation, including careful examination of the patient’s dental condition and a count of the number of teeth. Melhuish et al [8] reported misdiagnosis of a tooth in the lung after tracheal intubation. Repeated chest X-rays showed a molar in the bronchus. However, it was not retrieved until it was incidentally found at the end of an endotracheal tube’s suction catheter following extubation. Similarly, tooth loss and subsequent aspiration is often overlooked and considered difficult to detect without a high level of suspicion.
The 3 cases described in this case report also address the loss of dental bridges unnoticed during an ICU stay, each case with a slightly different clinical setting. In Case 1, the patient was bedridden and intubated, and could therefore not communicate the discomfort caused by the loss of the dental bridge. It was believed that the dental bridge did not pass through the gastrointestinal (GI) tract because he had a feeding tube for enteral nutrition and an endotracheal tube with an inflated balloon that prevented passage to the airway. Therefore, dental bridge had remained in the pharynx. In Case 2, the dental bridge also remained in the pharynx and was unable to pass through the GI tract due to the indwelling feeding tube. She was also unable to fully communicate with her physicians because of her drowsy mental status. In Case 3, the dental bridge had passed through to the stomach where delayed recognition that the bridge was missing had led to the need for endoscopic removal.
Chest X-rays revealed the loss of dental bridges in all 3 cases that were repetitively missed by ICU physicians and nurses. The ventilator-associated pneumonia bundle [9] has interventions for preventing ventilator-associated pneumonia, including oral hygiene management when using chlorhexidine. Likewise, management of the ICU patient’s oral health and dentition is essential. The hospital where this retrospective study was carried out provides a similar protocol. However, these protocols were not closely followed and each patient’s dental status was not checked, and so dental bridge losses occurred. Many patients already had poor oral hygiene with significant tooth loss, and it is easy to consider their oral hygiene as insignificant and neglect it.
The application of a detailed protocol is important for improving a patient’s oral health in the ICU. In 2011, a multicenter study examined the effects of systematic oral care in critically ill patients [10]. The study used the Beck Oral Assessment Scale which includes criteria for the lips, gingiva and oral mucosa, tongue, teeth, and saliva, and showed improvements after the implementation of a standardized protocol [10]. At Korea University Anam hospital more detailed protocols were subsequently developed, including a sketch of the patient’s dental condition (by the ICU nurse) which was passed on to the next ICU nurse at handover. Health care workers started to pay more attention to managing the oral cavity, including dental bridges. All 3 cases described in this case report resulted in quality improvements and further education for the health care workers. However, despite the new protocols, tooth loss has continued to occur; thus, we believe that dentists may be needed in the future to oversee the oral care of the many elderly patients with poor oral health conditions in the ICU.
In conclusion, careful examination of each patient’s oral cavity is essential to prevent potential deleterious complications. The number of teeth and the existence of dental prosthetics must be carefully documented.