Management of an Open Abdomen Considering Trauma and Abdominal Sepsis: A Single-Center Experience
Article information

Abstract
Purpose
To describe the experience of patients over a 7-year period who have had open abdomen (OA) surgery, at a tertiary university hospital.
Methods
The medical records of 59 patients, who were managed with OA after a laparotomy between March 2009 and December 2015, were reviewed retrospectively. The data collected included demographics, indication for OA, abdominal closure methods, abdominal closure rate, the intensive care unit stay duration, mechanical ventilation duration, hospital stay duration, and complications.
Results
Forty-seven patients (37 males, 78.7%) with a mean age of 52.2 ± 16.7 years were reviewed in the study. The indications for OA were traumatic intra-abdominal bleeding in 23 patients (48.9%), nontraumatic bowel perforation in 10 (21.3%), non-traumatic bleeding in 7 (14.9%), and bowel infarction in 6 (12.8%). The abdominal wall was closed in 38 patients (80.9%). Primary closures and fascial closure using an artificial mesh were performed on 21 (44.7%) and 12 patients (25.5%), respectively. The median number of dressing changes was 0 (interquartile range 0 - 1). The median duration of the intensive care unit and hospital stays were 12.0 and 32.0 days, respectively. The median interval to abdominal closure was 4 days (interquartile range 2 - 10.3 days). Twenty-seven patients developed complications, including uncontrolled sepsis (21.3%), entero-atmospheric fistula (19.1%), ventral hernia (8.5%), bleeding (4.3%), and lateralization (4.3%). The mortality rate was 44.7% with sepsis being the main cause of death (61.9%).
Conclusion
Traumatic intra-abdominal bleeding was a common indication for OA. Primary closure was performed in most patients, and frequent complications resulted in poor patient outcomes.
Introduction
In the supine position, intra-abdominal pressure is usually 0mmHg but can increase by up to 10mmHg following abdominal surgery [1]. Increased intra-abdominal pressure affects organ function in critically ill patients and may lead to abdominal compartment syndrome [2].
Open abdomen (OA) describes temporary abdominal wall closure when the skin and fascia have not been closed after a laparotomy [3]. When the fascia is intentionally left open to avoid elevation of intra-abdominal pressure following laparotomy, then surgical re-exploration is desirable. However, if the abdomen is opened for a long time, lateral retraction of the fascia can occur leading to closure difficulties, which complicate future abdominal surgery ,and increase patient morbidity and mortality [4].
However, in Korea there is limited data about the indications, complications, and time interval to abdominal closure of OA after a laparotomy. Therefore, the objective of this present study was to evaluate OA in a single-center tertiary university hospital, and examining whether non-traumatic patients with preoperative conditions like pre-repetitive operations and septic conditions, would cause worse results than those of traumatic patients.
Materials and Methods
The medical records of 59 patients at a tertiary university hospital who were managed with OA following laparotomy between March 2009 and December 2015 were reviewed retrospectively. Patients who died within 48 hours after the initial OA were excluded from the study. The study was approved by the Institutional Review Board (IRB no.: 4-2016- 1159), and informed consent was waived due to the retrospective nature of the study. All procedures were conducted in accordance with the Declaration of Helsinki.
Collected data included demographics, indications for OA, abdominal closure methods, abdominal closure rate, intensive care unit stay duration, mechanical ventilation duration, hospital stay duration, and complications. OA indications included traumatic hemoperitoneum requiring massive transfusion, uncontrolled intra-abdominal infection, bowel infarction requiring second-look laparotomy, and impending risk of abdominal compartment syndrome such as nontraumatic intra-abdominal bleeding. OA was maintained via temporary abdominal closure (TAC) and negative pressure wound therapy (NPWT; Figures 1 and 2). These techniques are used to treat postoperative wound complications, to prevent intra-abdominal wound infection, and for temporary wound closure after laparotomy [5].

Open abdomen – temporary abdominal closure.

Open abdomen – negative pressure wound therapy.
During maintenance of the OA, bowel and peritoneal membrane was detached using poly-vinyl sheets to prevent postoperative adhesion between bowel and peritoneal membrane, and to protect the bowel from the negative pressure injury. Small holes on the poly-vinyl sheet were made to enhance the drainage of fluid and blood during negative pressure. Two sheets were overlapped to the same cavity and to avoid direct negative pressure to the bowel accounting for the position of the holes in both sheets. These are the common principles of the TAC and NPWT.
In TAC, the surgical pad containing the suction tube was put on the sheets to create negative pressure, and one additional sheet was put into position to cover the whole abdomen.
NPWT is a sponge-based technique using commercially available products like CuraVAC (Cgbio Co., Seongnam, Korea) which contain sponge. The sponge placed on the two sheets in place of the surgical pad, with one more additional sheet placed on it covering the whole abdomen. The commercial suction kit was then put on the sponge for negative pressure.
Statistical analysis was performed using IBM SPSS Statistics ver. 23.0 (IBM Co., Armonk, NY, USA). Continuous variables were expressed as means and standard deviations or medians and interquartile ranges (IQR), and were compared between the groups using the Student t-test or Mann-Whitney U test. Categorical variables were expressed as n (%), and were compared between the groups using Fisher’s exact test. A p < 0.05 was considered statistically significant.
Results
There were 47 patients included in this study (Figure 3). The mean age was 52.2 ± 16.7 years, and 37 patients (78.7%) were male. The leading indication for OA was a traumatic abdominal injury in 23 patients (48.9%), followed by nontraumatic bowel perforation in 10 (21.3%; Table 1). Preoperative shock occurred in 37 patients (78.7%). The abdominal wall was closed in 38 patients (80.9%; Table 2). The median duration of intensive care unit and hospital stays were 12.0 (IQR, 5 - 26) and 32.0 (IQR, 15 - 69) days, respectively. The median interval to abdominal closure after OA was 4 days (IQR, 2 - 10.3 days) and the median number of dressing changes was zero (IQR, 0 - 1). The abdominal wall was closed mainly by primary closure in 21 patients (44.7%) and fascial closure using artificial mesh in 12 patients (25.5%; Table 3). Twenty-seven patients developed complications, including uncontrolled sepsis in 10 patients (21.3%), entero-atmospheric fistula in 9 (19.1%), and ventral hernia in 4 (8.5%; Table 3). Nineteen patients (40.4%) did not experience any complications. Twenty-one patients died, resulting in a mortality rate of 44.7%; with sepsis being the cause of death in 23 patients (48.9%), followed by nontraumatic bowel perforation in 10 (21.3%; Table 1). Preoperative shock occurred in 37 patients (78.7%). The abdominal wall was closed in 38 patients (80.9%; Table 2). The median duration of intensive care unit and hospital stays were 12.0 (IQR, 5-26) and 32.0 (IQR, 15-69) days, respectively. The median interval to abdominal closure after OA was 4 days (IQR, 2-10.3 days) and the median number of dressing changes was zero (IQR, 0-1). The abdominal wall was closed mainly by primary closure in 21 patients (44.7%) and fascial closure using artificial mesh in 12 patients (25.5%; Table 3). Twenty-seven patients developed complications, including uncontrolled sepsis in 10 patients (21.3%), entero-atmospheric fistula in 9 (19.1%), and ventral hernia in 4 (8.5%; Table 3). Nineteen patients (40.4%) did not experience any complications. Twenty-one patients died, resulting in a mortality rate of 44.7%; sepsis and septic shock were the main cause of death (Figure 4).
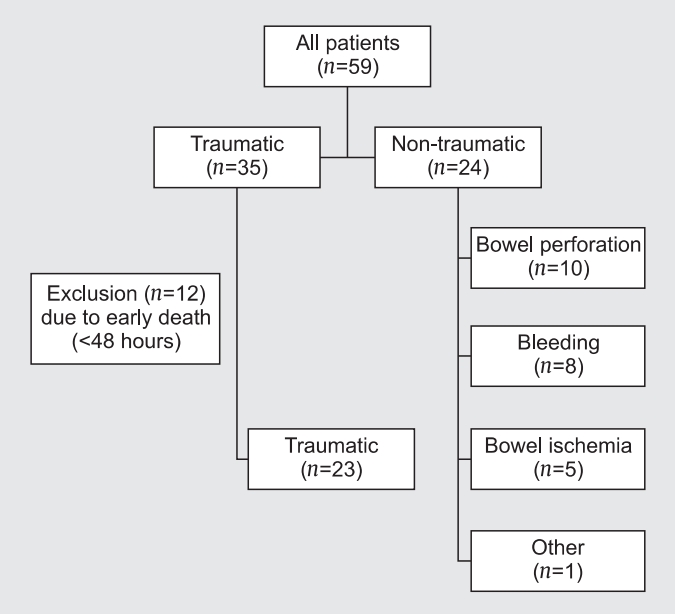
Flow chart of study population.

Patient characteristics.
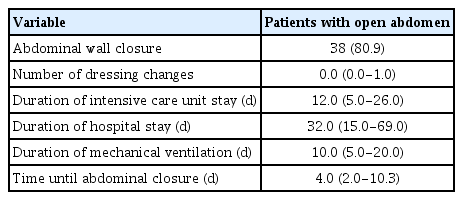
Characteristics of open abdomen.
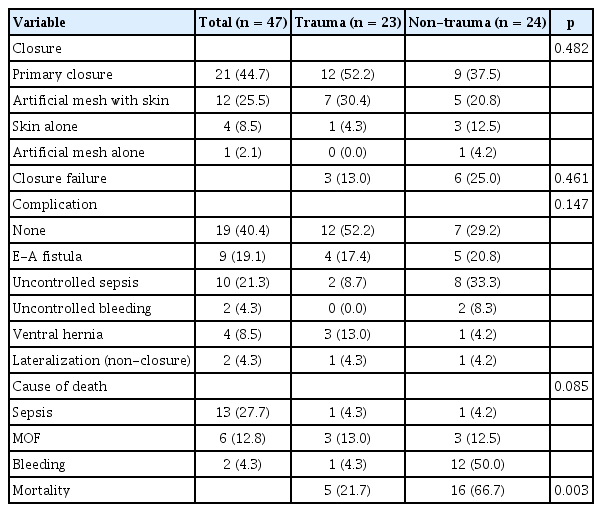
Methods of abdominal wall closure, closure failure, complications, cause of death and mortality of open abdomen.
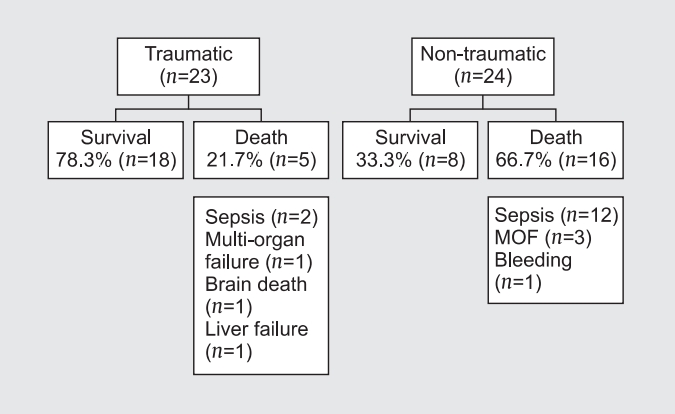
Causes of mortality. MOF indicates multi-organ failure (p = 0.002). MOF = multi-organ failure.
There were no significant differences in the closure rates between traumatic OA and non-traumatic OA (86.9% versus 75%, respectively; p = 0.298). However, survival rates were significantly different between traumatic OA and nontraumatic OA (73.9% versus 33.3%, respectively; p = 0.002).
Discussion
Although OA can lead to complications such as enterocutaneous fistula, ventral hernia, uncontrolled bleeding, and sepsis, it is a recommended strategy to treat critically ill patients [6-10]. Early fascial closure is important for shorter hospital stays and lower rates of complications [11].
Seternes et al [12] assessed the effectiveness of NPWT and found that fascial closure was performed in two-thirds of cases. Interestingly, both Acosta et al [13] and Rasilainen et al [14] combined a mesh method with the negative pressure technique, achieving fascial closure rates of 76% to 78%. Other studies have shown closure rates varying from 68% to 100% [15-21]. The results of these previous studies are congruent with the findings of the present study, in which the total rate of fascial closure was 80.9%. Fascial defects were repaired by direct closure in 44.7% of patients and by artificial mesh in 27.7% of the patients.
Lateralization occurs in all patients if OA is maintained for a long time, mainly associated with intra-abdominal hypertension which may lead to closure failure. There are some medical strategies avoiding intra-abdominal hypertension like fluid restriction, avoiding hypothermia, nasogastric drainage, insertion of rectal cannula, administration of prokinetic agents, endoscopic decompression, and using colloids or hypertonic solutions [22].
Fascial closure rates are lower in patients undergoing OA because of poor medical conditions (non-traumatic) compared with those undergoing OA due to trauma [23], and sepsis was noted as a major indication for medical OA. A similar pattern was observed in the present study, and even in patients with traumatic OA, sepsis was the main cause of complications and death. The fascia was not closed in 3 of 5 patients who died following traumatic OA, and in 6 patients of 16 expired patients with non-traumatic OA. The main cause of closing failure seems to be connected with mortality, however, statistical analyses did not demonstrate any significant factors associated with closing failure. Quyn et al [24] found that multi-organ failure (MOF) was the principal cause of mortality and argued that this might be due to primary or secondary complications such as fistula formation or intestinal leakage, either of which could cause sepsis and multi-organ failure. The same patterns regarding causes of mortality were also expected in the present study. In addition to a patient’s general condition, bowel problems such as fistula, anastomosis site leakage, and free perforations are strongly associated with mortality [25]. Although these bowel problems can occur in patients treated using a negative pressure closure system, Rao et al [10] warned of the dangers of using negative pressure closure. Therefore, care is required when performing dressing changes to avoid the need for further surgery due to bowel edema or adhesion [26,27].
The difference in mortality rates between traumatic and nontraumatic OA might be due to different preoperative conditions. In many patients with traumatic OA, their general condition and intra-abdominal pressure were at least equivalent to those in patients with non-traumatic OA, so mortality rates among patients with traumatic OA may be lower. Mortality of traumatic patients within 48 hours showed acute coagulopathy and uncontrolled bleeding as the major causes, suggesting that early hemodynamic instability from multiple traumas such as pelvic bone fracture and major vessel injury may be involved. In contrast, mortality of non-traumatic patients shows a different pattern. In 12 of 16 patients, sepsis was the main cause of death. And the sepsis was associated with preoperative anastomotic leakage or repeated postoperative bowel perforation. Trauma patients who died within 48 hours after OA were excluded from the study because we could not evaluated the success rate of OA. So, in non-trauma patients, mortality rate was higher than trauma patients.
In 2016, Osvaldo et al proposed that OA and negative-pressure techniques improved the care of patients with traumatic OA, but stressed that closure must be achieved early to avoid complications [28]. Early definitive closure of fascial defects is one of the most important factors for complication prevention [29]. In the present study, in patients with traumatic OA, there was a strong relationship between closure failure and mortality, but this association was not observed in patients with non-traumatic OA.
It is expected that complications would be strongly associated with mortality, but that preoperative conditions would be the strongest risk factor for mortality in patients with non-traumatic OA. The majority of patients with non-traumatic OA were transferred from other departments including the departments of urology, gynecology, and colorectal surgery, owing to unstable conditions such as uncontrolled bleeding or sepsis following cancer surgery. Therefore, most patients had a high mortality risk before OA. After transfer, damage control surgery such as bleeding vessel ligation, and primary closure of perforated bowel was applied using OA. Therefore, the poor preoperative conditions are likely to be the main causes of the high mortality rates observed in patients with non-traumatic OA.
It is very hard to point out what was the main cause of MOF, especially with complex, systemic septic conditions. Anastomosis site leakage, bowel fistula and uncontrolled sepsis appeared to be the main causes of MOF, but pneumonia happened secondarily, with uncontrolled sepsis being an additional cause of MOF (Table 3).
The present study had limitations due to the retrospective design and small number of participants. In addition, because of heterogeneity among the participants, a subgroup analysis would be needed to uncover other potential relationships between risk factors and mortality. The statistical analysis of factors associated with closing failure is difficult. There was no significant factor affecting the closure failure. Large-scale, prospective, multicenter studies including subgroup analyses would provide a more comprehensive overview of the risk factors associated with mortality in patients with OA.
In conclusion, in this single-center setting, traumatic intra-abdominal bleeding was a common indication for OA. Primary closure was performed in most patients, and OA was feasible for the management of traumatic and non-traumatic indications. However, OA was associated with multiple complications and high mortality rates, especially in nontraumatic patients. Further studies are needed to develop more effective strategies for controlling sepsis in patients with nontraumatic OA.
Notes
No potential conflict of interest relevant to this article was reported.
Acknowledgements
The authors wish to thank KW Lee for assistance with the statistical analyses and all of the coordinators for their valuable help and cooperation. This research was supported by a faculty research grant from the Yonsei University College of Medicine (6-2016-0100).
This abstract was presented orally at the Critical Surgical Abdomen Consensus Conference, held on July 22-23, 2016, in Dublin, Ireland.