Introduction
Transanal evisceration of the small bowel is an extremely rare surgical emergency. Rectal perforation in such cases is usually due to an underlying rectal prolapse. Spontaneous rectal perforation has been reported in elderly patients with a history of chronic constipation, or malignancy of the rectum or colon. It may also be a complication of other rectal diseases such as diverticulitis, blunt or penetrating trauma, or the spontaneous rectal perforation may be iatrogenic (caused during instrumentation). Near total small bowel evisceration through the anal canal following spontaneous rectal perforation is an extremely rare event in an otherwise healthy male.
Case Report
A 45-year-old, otherwise healthy male presented as a surgical emergency with complaints of loops of small bowel coming out through his anus following defecation. The patient had developed lower abdominal pain, but had no prior history of rectal prolapse, chronic constipation, altered bowel habits, rectal bleeding, or trauma. On examination, the patient was conscious, afebrile, had tachycardia (100 bpm), and a blood pressure of 110/60 mmHg. His abdomen was soft, not tender, distended, or rigid, and the patient was not guarding. The majority of the small bowel (more than 150 cm) had come out of the rectum (which was congested). Barring leukocytosis (with total leukocyte count of 13,500/ÎźL), other laboratory results (prothrombin time, serum albumin, serum lactate, renal and hepatic function tests, and arterial blood gas analysis) revealed values in the normal range. The patientâs condition necessitated immediate surgical intervention due to the risk of gangrene in the eviscerated bowel segment and the associated high mortality in such cases. This precluded the use of preoperative radiological investigation.
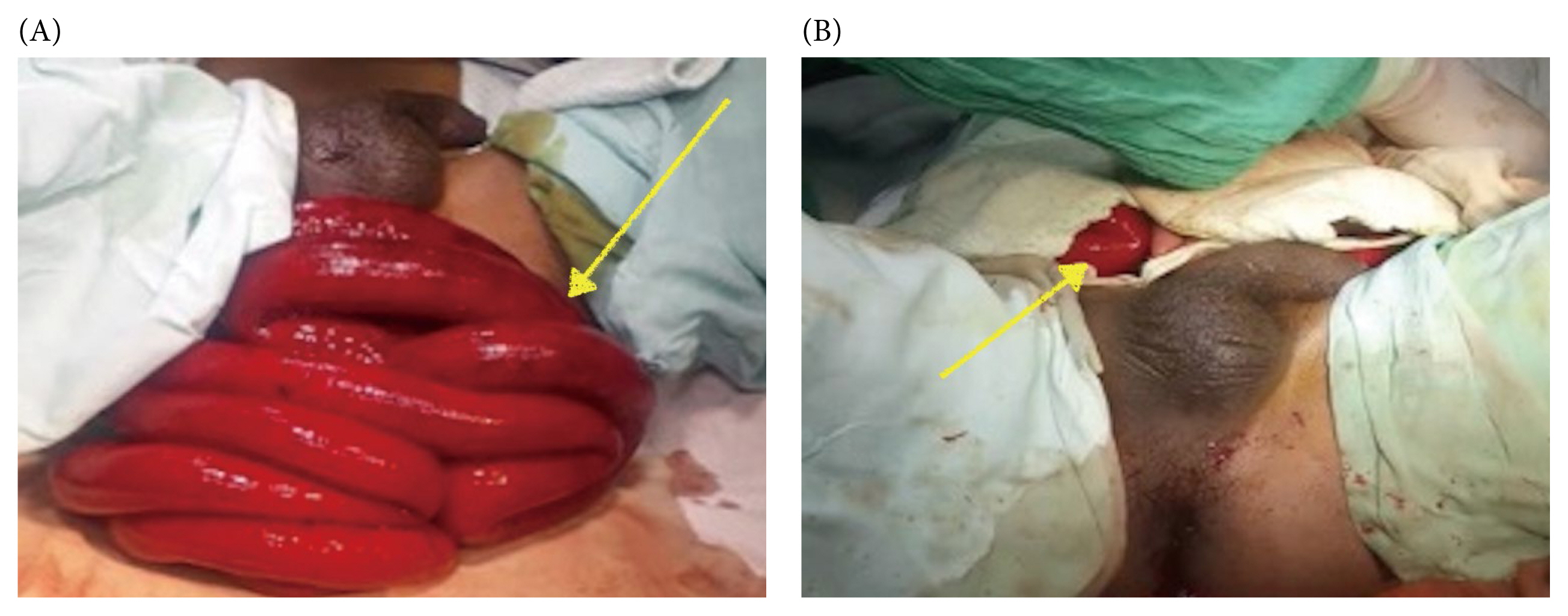
With continued initial resuscitation, the patient was taken for abdominal exploration (about 4 hours after the onset of symptoms) which was performed using a midline laparotomy under general anesthesia. Approximately 150 cm of extruded small bowel (Figure 1A) were reduced through the rectosigmoid tear and placed in the peritoneal cavity (Figure 1B). A 5 cm irregular longitudinal tear was observed about 8â10 cm above the anal verge, without thickening or ulceration, and the tear was along the anterior aspect of rectum involving the rectosigmoid junction through which almost the whole of the small bowel loops had eviscerated (Figure 2). There was no growth or diverticula of the colon, rectum, or anal canal, and no fecalith or foreign bodies identified. The whole of the small bowel was repositioned in the abdominal cavity and was deemed viable. Considering the patientâs age, minimal physiological derangements, and lack of evidence of small bowel necrosis or intraperitoneal fecal contamination or sepsis, the rectal tear was repaired in 2 layers using polyglactin 3-0 sutures, followed by insertion of a single abdominal drain in the pelvic cavity. Post reposition of the small bowel, the anal opening was examined, and no evidence of rectal prolapse or anal sphincter defect was identified. Abdominal closure was performed in 2 layers using polypropylene 1-0 for the fascia and nylon 1-0 for the skin. The post operative course was uneventful and so the patient was allowed liquids from the 2nd post operative day, with full oral intake by the 4th postoperative day. The drain was removed on the 5th postoperative day, antibiotics were prescribed for 7 days (3rd generation cephalosporin and metronidazole), and the patient was discharged on the 8th postoperative day. There was no obvious pathology observed during the lower gastrointestinal endoscopy following 6 months of uneventful surgical outpatient clinic appointments.
Discussion
Transanal evisceration of the small bowel is a rare event; however, many cases have been reported since the 1st description of this condition by Brodie in 1827. Spontaneous rectal rupture with small bowel evisceration is also a rare clinical entity [1â5]. Perforation of the rectum or the rectosigmoid usually occurs due to acute or chronic ulceration of the intestinal wall. The etiology of the ulcer in most cases is diverticulosis, solitary rectal ulcer, or malignancy. The rectum or rectosigmoid can rupture due to a sudden increase in intrabdominal pressure which usually occurs due to blunt abdominal injuries, and rarely occurs in cases of sudden heavy lifting, or by chronic straining during defecation in chronically constipated individuals. The term âspontaneous ruptureâ is used when no specific etiology can be ascertained. The proposed mechanisms of rupture in these cases include intramural hemorrhage with the hematoma separating and weakening the rectal wall, congenital annular malformations causing a rectal weak spot, or a progressive deepening of the pouch of Douglas with a sudden increase in intra-abdominal pressure [6â8]. The standard management strategy involves an exploratory laparotomy, abdominal cavity irrigation, repositioning of the small bowel, and suturing of rectal wall [9]. In another reported case of spontaneous rectosigmoid rupture with an acute transanal small bowel evisceration, the patient was managed by laparoscopic suture repair of the rectosigmoid perforation site after repositioning of the small bowel in the abdominal cavity without the use of a stoma [2]. We propose that the initial emergency treatment must include an immediate attempt to reduce the eviscerated bowel, along with repair of the perforation site (with a requirement for a defunctioning bowel stoma in frail patients with intraabdominal collection/sepsis and risk/established bowel ischemia, to prevent leakage at the site of suture repair and the associated morbidity).
Small bowel evisceration through the anal verge is an emergent condition requiring surgical intervention and finding the cause of the evisceration should be sought after surgical management to prevent recurrence or sepsis related life threatening complications.