Introduction
Pyometra is a rare condition which was defined in 1981 as the accumulation of purulent material in the uterine cavity because of an obstruction of the natural drainage of the uterus [1]. The accumulation of pus in the uterine cavity causes a rapid progression of necrosis which may exert pressure on the weakened uterine wall, and lead to spontaneous perforation of the pyometra which may result in spontaneous pneumoperitoneum [2], however, this is rare (0.01–0.05%) [3]. If a pyometra ruptures, the patient typically develops acute abdominal and generalized peritonitis, increasing the risk of mortality. In this case report, pneumoperitoneum and diffuse peritonitis caused by spontaneously perforated pyometra is described in a patient who was preoperatively diagnosed and successfully treated by emergency laparotomy.
Case Report
An 80-year-old woman visited the emergency department with a 3-day history of diffuse abdominal pain and nausea. She had a history of hypertension and diabetes for which she had been taking medication for 10 years. Her vital signs were: blood pressure of 110/70 mmHg, heart rate of 100 beats/minute respiratory rate of 20 breaths/minute, and body temperature of 37.2°C. On physical examination, her abdomen was slightly distended, with direct tenderness and rebound tenderness of the entire abdomen. A vaginal examination showed no cervical or vaginal anomalies, and there was no vaginal discharge or abnormal fluid in the cavity. Initial laboratory results revealed that her white blood cell count was 20,130/μL, C-reactive protein level was > 42 mg/dL, procalcitonin was >100 ng/mL, and lactic acid level was 4.0 mmol/L. Computed tomography (CT) scans showed the presence of free intra-abdominal air, a fluid-filled uterus with internal air foci, and a focal wall defect at the right anterior aspect of the uterus (Figure 1).
After prompt fluid resuscitation and intravenous antibiotics, an emergency laparotomy was performed to identify the cause of the intra-abdominal free air. (Spontaneous perforation of a pyometra was suspected).
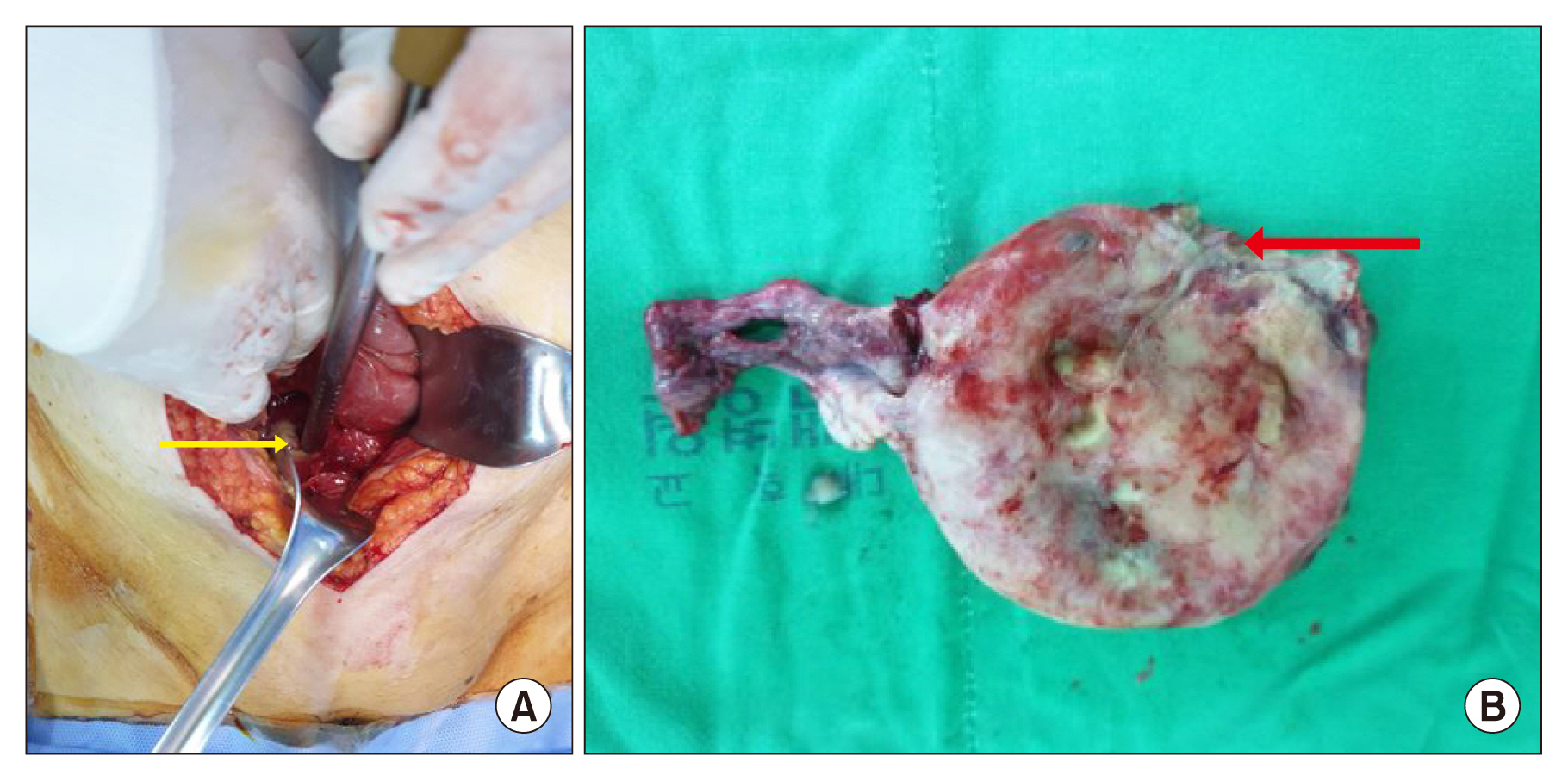
Copious purulent fluid was observed in the peritoneal cavity which was draining from a perforation measuring 2 cm in diameter in the fundus of the uterus (Figure 2A).
The uterus exhibited focal necrosis and a perforation in the fundus but showed no evidence of malignancy (Figure 2B).
Furthermore, other abdominal organs appeared unremarkable. A total abdominal hysterectomy was performed by a gynecologist. The patient was admitted to the intensive care unit and received intravenous broad-spectrum antibiotics [piperacillin/tazobactam (4.5 g every 6 hours) and metronidazole (500 mg every 8 hours)]. Enterococcus faecalis was isolated from the abdominal pus. Histological examination revealed acute pyogenic inflammation in the uterus involving the cervix, endometrium, myometrium, and parametrium, with perforation and focal necrosis. Although she persisted with a fever which spiked, her condition improved, and she was transferred to the general unit on Postoperative Day 3. Oral food intake was initiated with sips of liquid on Postoperative Day 4 and gradually progressed to a solid diet. On Postoperative Day 10, a follow-up CT scan was performed and revealed no abnormalities. She was transferred to another hospital on Postoperative Day 16 without complications.
Discussion
Pneumoperitoneum is defined as the presence of free air within the peritoneal cavity [4]. In general, more than 90% of the cases of pneumoperitoneum are caused by gastrointestinal tract perforation [5]. However, pneumoperitoneum may occur without a perforated viscus (“non-surgical” or “spontaneous” or “misleading” pneumoperitoneum).
Spontaneous pneumoperitoneum is associated with intrathoracic, intraabdominal, gynecological, iatrogenic, or other miscellaneous cases (Table 1) [4,5]. Spontaneous pneumoperitoneum in the peritoneal cavity, detected during radiological examination that is not caused by viscus perforation and not requiring surgical intervention, is observed during a laparotomy [5].
Spontaneous pneumoperitoneum that is not due to gastrointestinal perforation and is caused by spontaneous perforation of a pyometra is a condition where there is an accumulation of pus in the uterine cavity due to an obstruction to the natural drainage of the uterus [1]. A pyometra is reported to occur in 0.1–0.2% of all gynecology patients, of which 13.6% are elderly women [6]. The accumulation of purulent material in the uterine cavity with compromised natural drainage, leads to the thinning of the uterine walls, which can cause perforation of the pyometra and spontaneous pneumoperitoneum when under pressure [4]
Pneumoperitoneum due to the perforation of spontaneous pyometra, which is one of the gynecologic causes of these spontaneous pneumoperitoneum, rarely occurs and comprises of 0.01–0.05% of all cases [3]. The most common presenting symptoms are lower abdominal pain, purulent vaginal discharge, and postmenopausal vaginal bleeding [7]. Symptoms of pyometra may be non-specific; more than 50% of pyometra cases remain asymptomatic, resulting in a delayed or missed diagnosis [8]. Thus, a definitive diagnosis of pyometra preoperatively is challenging and may, subsequently lead to an increased risk of perforation of the pyometra [7,9]. Once the pyometra has ruptured, the patient develops acute abdominal and generalized peritonitis. These conditions cause an increase in the morbidity and mortality of spontaneously perforated pyometra. Therefore, most cases often require prompt emergency surgical intervention [3]. Septic shock is potentially a life-threatening complication [10]. Management of pyometra depends on the patient’s clinical status (emergency or nonemergency) and the status of pyometra (ruptured or unruptured). Urgent cases of ruptured pyometra should be managed by emergency laparotomy, irrigation of peritoneal cavity, hysterectomy, and administration of broad-spectrum antibiotics [11].
In conclusion, although pneumoperitoneum caused by pyometra perforation is considered to be spontaneous peumoperitoneum, delayed diagnosis and treatment may result in an increase in morbidity and mortality. Therefore, aggressive treatment is needed, including surgery, postoperative intensive care support, and administration of antibiotics. If an elderly woman presents with pneumoperitoneum, vague abdominal pain, and gynecological symptoms, acute care surgeons should be mindful of the possibility of pyometra perforation.