Antimicrobial Management of Complicated Skin and Soft Tissue Infections in an Era of Emerging Multi-Drug Resistance: Perspectives from 5 Gulf Countries
Article information

Abstract
The number of complicated skin and soft tissue infections (cSSTIs) in the Arabian Gulf region has risen in recent years, particularly those caused by multi-drug resistant (MDR) pathogens. The high prevalence of diabetes, obesity, and associated cardio-metabolic comorbidities in the region renders medical and surgical management of cSSTI patients with MDR infections challenging. An experienced panel of international and regional cSSTI experts (consensus group on cSSTIs) was convened to discuss clinical considerations for MDR infections from societal, antimicrobial stewardship, and cost perspectives, to develop best practice recommendations. This article discusses antibiotic therapies suitable for treating MDR cSSTIs in patients from the Gulf region and recommends that these should be tailored according to the local bacterial ecology by country and region. The article highlights the need for a comprehensive patient treatment pathway and defined roles of each of the multidisciplinary teams involved with managing patients with MDR cSSTIs. Aligned and inclusive definitions of cSSTIs for clinical and research purposes, thorough and updated epidemiological data on cSSTIs and methicillin-resistant Staphylococcus aureus in the region, clear-cut indications of novel agents and comprehensive assessment of comparative data should be factored into decision-making are necessary.
Introduction
Complicated skin and soft tissue infections (cSSTIs) comprise a wide group of infections with diverse microbiological causes. These infections may affect the superficial dermis, subcutaneous tissue, fascia, or muscle, and presentation can range from simple superficial infections to severe necrotizing infections [1,2]. Mild infections typically present with local signs and symptoms, such as redness and swelling, and can often be managed with incision and drainage. Moderate-to-severe infections often present with both local, and systemic manifestations including pyrexia, tachycardia, tachypnea and/ or leukocytosis, and require surgical intervention, including source control, and antimicrobial therapy [2,3]. For all types of infection, determining the causative pathogen(s), and whether the infection is monomicrobial or polymicrobial is essential for recommending appropriate antibiotic treatment. Managing larger wounds in patients with co-morbidities requires specialized care from a multidisciplinary team (Figure 1) [2,4–6].

Characteristics of complicated skin and soft tissue infections according to patient, wound specific factors and causative pathogen.
Robust definitions for cSSTIs are vital for capturing the broader spectrum of these infections and assessing the appropriate treatment. The 1st challenge with the clinical management of cSSTIs is the inconsistencies between the definitions used in published literature and guidelines [3,5]. The 2013 update of the (1998) US Food and Drug Administration guidance defines acute bacterial skin and skin structure infection as a wound infection, erysipelas/ cellulitis, and major cutaneous abscess (Table 1) [7]. While this more closely defines cSSTIs for the registration of trials than the earlier guidance, it is still limited because it excludes many types of infections (e.g., necrotizing fasciitis, infected pressure ulcers, pyomyositis, furuncles, and carbuncles) [7]. The Infectious Diseases Society of America guidelines [2] categorize infections by tissue necrosis (necrotizing versus non-necrotizing), as well as purulence (purulent versus non-purulent), and severity (mild, moderate, and severe). From a clinical standpoint, the differentiation of severity is essential as it guides surgical, and antibiotic treatment decisions. The World Society of Emergency Surgery and Surgical Infection Society guidelines [1] also recommend defining the anatomical extension of the infected area, as well as independent clinical assessments of the patient. Aligned definitions are important from the outset because it can be difficult to recognize which infections require immediate attention and intervention, and allows the differentiation of these infections from less severe infections.
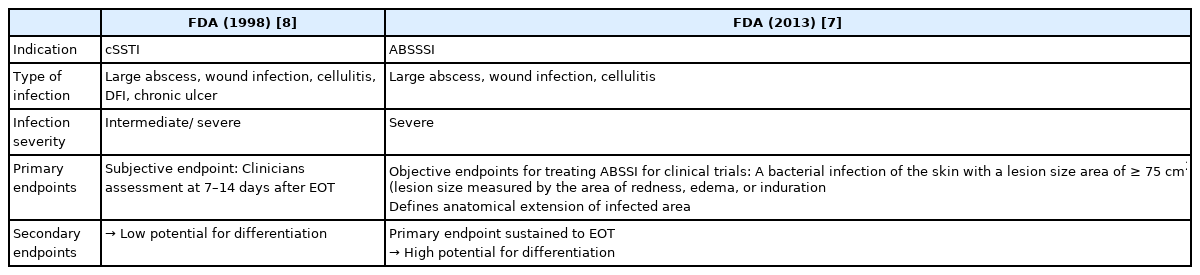
Overview of updated FDA guidance on SSTI.
Responsible for a large proportion of infections that require hospitalization, cSSTIs can threaten life and limbs, causing significant morbidity and mortality [6]. Clinical management of cSSTIs requires a multidisciplinary approach, and clinicians must consider patient-specific features including the type of infection and severity, as well as previous exposure to cSSTIs and antibiotic use. The presence of comorbid conditions, such as diabetes, obesity, critical illness, immune compromise, liver and kidney disease, and vascular insufficiency often worsens outcomes [8], and indeed, whether a patient will be hospitalized or not [9]. Among modifiable risk factors, obesity has been reported to increase the risk of recurrent cSSTIs [10] and smoking has been reported to increase the risk of surgical-site infections in elective plastic surgery patients [11]. Both smoking and obesity have been reported to increase the risk of surgical-site infections in women undergoing a cesarean delivery [12,13].
In this review article, the key principles of the management of cSSTIs in 5 Gulf countries (Bahrain, Kuwait, United Arab Emirates (UAE), Oman, and Qatar) are discussed with a focus on current treatment practices, barriers to optimal treatment, and local differences (where data are available). The different therapies available are considered and steps that could be taken to optimize the diagnosis and treatment of cSSTIs in this region are highlighted.
Materials and Methods
As clinical decision-making in the management of cSSTIs can vary significantly between regions across the globe, the Gulf Consensus Group on complicated skin and soft tissue infections (GCG-cSSTIs) convened to provide experience-based opinions on cSSTI diagnosis and management in the region. This panel was comprised of experts in the field from Bahrain, Kuwait, UAE, Oman, and Qatar who were chosen on the basis of their contributions and roles in their national societies. The group was guided by Prof. Dr. Christian Eckmann, who is an expert in the field of cSSTIs. The panel included microbiologists, infectious disease specialists, and surgeons, some of whom are intensivists in their affiliated institutions.
Panel members received a pre-meeting survey comprising of questions designed to understand their clinical experience and their approach in treating cSSTIs. The results of the survey were presented at a meeting in Kuwait. During the meeting, the panel discussed current microbiological and epidemiological trends, existing antibiotics, and local and international guidelines for the treatment of cSSTIs in the 5 Gulf countries. The overarching goal was to outline unmet needs providing cSSTI management and treatment options which were applicable to the 5 Gulf countries studied. The insights communicated at the meeting were summarized and shared with the participants following the meeting.
A review article thus developed was extensively, critically reviewed by the panel members and the comments were addressed.
1. Epidemiology, microbiology, and antimicrobial resistance
Understanding landscape epidemiology is of great importance. By determining local antibiotic resistance patterns and typical causative pathogens, treatments, and patient outcomes can be optimized. Gram-positive bacteria are predominant in cSSTIs (up to 80%), however, treatment is becoming ever more challenging owing to increased antimicrobial resistance [14]. Globally, Staphylococcus aureus, Streptococcus spp. and Enterococcus spp. are typically the 1st, 2nd and 3rd most common causative pathogens in cSSTIs, respectively [15,16]. Although, the spectrum of pathogens causing cSSTIs is becoming increasingly complex, and includes both hospital-acquired (HA) and community-acquired (CA) organisms, which have different epidemiology, antibiotic susceptibility, and microbiological properties [17,18]. Added to this, the escalating prevalence of antibiotic-resistant microorganisms causing surgical site infections presents a huge hurdle in the healthcare setting. The burden of SSTI is substantial, both economically, and societally, and includes complex infections such as those caused by methicillin-resistant S. aureus (MRSA) and more recently, multi-drug resistant Gram-negative bacilli [19,20]. Such complex infections are more likely to result in longer hospital stays and subsequent direct costs of hospitalization, staffing, barrier measures, and medication. Other aspects of patient care, such as managing anxiety, depression, and loss of autonomy, are no less important.
1.1. Epidemiology: A view from Bahrain, Kuwait, UAE, Oman, and Qatar
A Qatar surveillance system report published in 2011, observed that SSTIs were more common in Qatar than in Europe, with rates of 18.5% in Qatar versus 4.8% in Europe [21]. SSTIs represent a significantly large proportion of all infections; a 2019 study in Oman reported that 45% of processed samples obtained from urine and soft tissue collected in surgical wards and critical care areas, were SSTIs, with over half of these caused by Gram-positive bacteria [22]. While the data suggest a high prevalence of cSSTIs for the region, accurate epidemiological data are needed to ascertain the extent of the prevalence of different cSSTIs between and within countries in the region.
1.2. Specific risk factors for cSSTIs in Bahrain, Kuwait, UAE, Oman, and Qatar
Although the reason for such a high rate of cSSTIs is not fully understood, countries within the Gulf Cooperation Council (Bahrain, Kuwait, UAE, Oman, Qatar, and Saudi Arabia) have reported high rates of diabetes mellitus in adults [23]. The world’s highest age-adjusted comparative prevalence of diabetes in 2019 (12.2%) according to the International Diabetes Federation regions of the world was reported in the Middle East and North Africa region [24]. Given that the prevalence of cardiometabolic conditions are key risk factors for developing cSSTIs, along with increasing age, and cancer [2,5,6], these comorbidities could, in part, be driving the cSSTI rate in the region, as reported in a study in Kuwait [25]. Diabetes is also associated with an increased likelihood of polymicrobial infections, more complex infections, and SSTI-related hospitalization [26,27]. Accordingly, guidance on blood glucose control and weight reduction prior to planned surgery is advised [25]. Risk factors may differ between populations in Bahrain, Kuwait, UAE, Oman, and Qatar, and other regions, reflecting population demographics including alcoholism, liver cirrhosis, human immune deficiency virus infection, and immunosuppression which are all risk factors observed in Europe as being associated with developing SSTIs, but these risk factors are not widely observed in Bahrain, Kuwait, UAE, Oman, and Qatar [28].
These data paint an incomplete picture; there are limited published data on the clinical management of associated cSSTIs in Bahrain, Kuwait, UAE, Oman, and Qatar, and causative pathogens are typically underreported, which may preclude the selection of the best treatment strategies. Robust, large-scale epidemiological studies using aligned classifications are needed. Although the Global Antimicrobial Resistance Surveillance System has been developed to facilitate accurate identification of worldwide trends and comparisons, it is limited and it does not cover all drug resistance and bacterial pathogens. Moreover, not all countries have participated. We propose the inclusion of all Gulf countries into such programs. In addition, the implementation of unified local registries could potentially support treatment optimization along with the collection of hard data on the organisms causing infections, demography, risk factors, and patient outcomes according to treatment.
1.3. MRSA in Bahrain, Kuwait, UAE, Oman, and Qatar
MRSA continues to be a leading cause of morbidity and mortality among hospitalized patients, particularly in those who are critically ill. In contrast to the European trend where there is a reduction in the prevalence of MRSA strains [29], the recent rise in antibiotic resistance among causative pathogens, particularly MRSA, has complicated the management of cSSTIs in the 5 Gulf countries. Data from these 5 Gulf countries has shown that in 2013 MRSA infection and colonization rates were moderate-to-high [30], however, the range varies widely between the 5 countries, and over time (Table 2 [30–40]). Data from UAE shows that 23–30% of culture isolates are identified as MRSA positive [31,32]. A meta-analysis in 2013 investigating MRSA colonization across Africa and the Middle East region showed an average MRSA colonization rate of 15.5% (13.4–17.6%) and a crude mortality rate of 44% [30]. Additionally, it should be noted for context that many of the published studies from the 5 Gulf countries preselected MRSA isolates without reporting their total prevalence in relation to other pathogens, meaning that the true proportion of MRSA isolates (of the total S. aureus isolates) is likely to be greatly underrepresented [33–35].
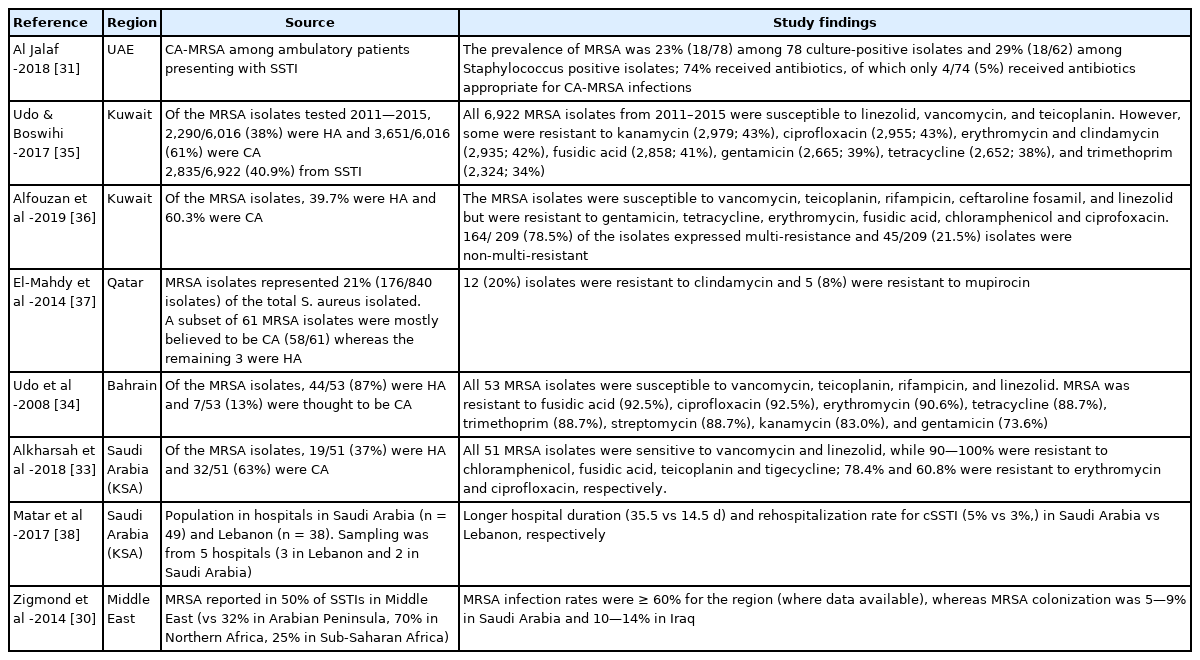
Summary of studies investigating cSSTIs and MRSA in 5 Gulf countries.

Previously confined to healthcare settings, MRSA strains are frequently the source of infection in community settings in the 5 Gulf countries. Studies report varying rates for CA-MRSA infections over time: in Kuwait and Saudi Arabia, CA-MRSA comprised of about 60% of infections [33,35,36]; and 90% in Oman [41]. A recent publication in 2020 by Udo et al [42] reported the emergence, and transmission of a previously rare CA-MRSA clone in Kuwaiti hospitals. In contrast, 1 study from Bahrain reported more HA-than CA-MRSA, although this earlier study published in 2008 [34] may include a different patient demographic, and may also reflect the status quo prior to the shift in MRSA source in recent years [43].
Risk factors for developing MRSA may differ, depending on whether the infection was HA or CA (Table 3 [15,40,44]). Overall, the MRSA prevalence in the Gulf countries appears to be higher than in many European countries [30].
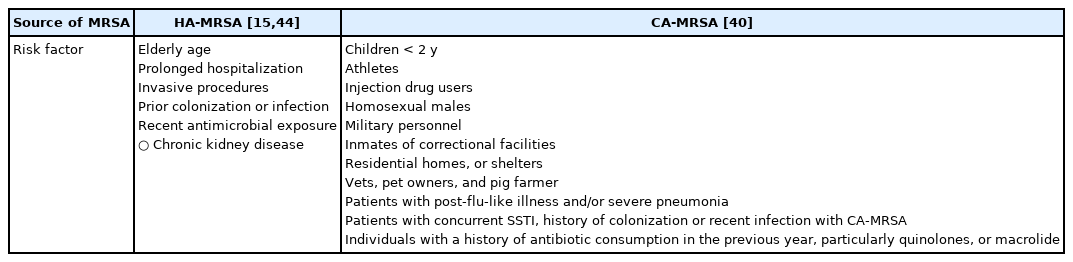
Risk factors for H-or CA-MRSA.
1.4. MRSA resistance and susceptibility data
Across the 5 Gulf countries, MRSA has been shown to be resistant to many antimicrobials used to treat SSTI, including fusidic acid, ciprofloxacin, erythromycin, tetracycline, trimethoprim, streptomycin, kanamycin, and gentamicin (Table 2). In a recent study in 2019 by Alfouzan et al [42] 58% of all MRSA isolates from Kuwait were reported to have a minimum inhibitory concentration > 1 μg/mL for vancomycin, which is associated with clinical failure of the drug. Although MRSA has been widely reported to be susceptible to teicoplanin, Alkharsah et al [33] in 2018 reported MRSA resistance to this agent, which limits treatment options for patients with renal failure. An added concern for clinical microbiologists is the reliability of susceptibility testing and interpretation. For example, tigecycline is associated with a higher likelihood of inconsistent results from automated antimicrobial susceptibility testing platforms [45]. Given that MRSA rates are rising, as observed in Kuwait [43], accurate epidemiological and surveillance data on cSSTIs in the 5 Gulf countries are needed to permit optimal management of patients with cSSTIs, including regular surveillance of MRSA for detecting the newly emerging clones. While informative, the regular susceptibility data submitted by hospitals are limited and more granularity is needed; for instance, comprehensive hospital data of types of cSSTIs should be made available from all the countries in the region.
1.5. Diagnosis and rapid testing
Identifying and addressing MRSA as early as possible has far-reaching effects on clinical outcomes, particularly because patients with more complex or severe cSSTI, or risk factors, are slower to respond to treatment [46]. It has been reported in 2020 that inappropriate treatment occurs in 40% of STTI cases [19], which has repercussions on patient outcomes; in 2007 Szumowski et al [47] reported a 6-fold increase in the probability of treatment success when MRSA is initially treated, versus delayed identification; yet worryingly, failure rates of (initial) empiric treatment can be as high as 20–40% versus targeted treatment [46,48–51].
Furthermore, inappropriate treatment is a significant risk factor for treatment failure [52], and is reportedly twice as common in mixed (Gram-positive, Gram-negative and anaerobes) infections [53]. Treatment failure is also associated with females, cardiovascular disease, high Body Mass Index, presence of cellulitis, inadequate empiric therapy and disease severity, inadequate or delayed surgical source control, extended hospital stays and associated costs [46,50,51], as well as an increase in reported fatalities [48,49].
Novel and rapid molecular methods of detecting pathogens from blood cultures in cSSTIs in 2006 offered the promise of reducing morbidity by controlling infection and guiding appropriate antimicrobial choice [49,54]. Molecular MRSA screening methods developed over a decade ago, have high sensitivity and rapid turnaround times but are not currently employed universally, owing to their associated high costs and inconsistent evidence regarding their impact on patient outcomes [55,56].
Cell culture is a common technique for MRSA surveillance [57] despite its longer turnaround times. In this regard, Montravers et al [58] reported that for non-necrotizing infections, blood cultures were positive in less than 5% of cases, and Al Jalaf et al [31] reported that only 78% of cSSTI had positive cultures, thus underpinning the need for more studies to establish the role of novel diagnostic technologies in SSTIs.
1.6. Treatment options against MRSA
The high rate of MRSA infections in the 5 Gulf countries studied warrants careful consideration of the available anti-MRSA options. In the last decade, several agents for treating MRSA, have become available, such as ceftaroline, ceftobiprole, telavancin, oritavancin, dalbavancin, tedizolid, and delafloxacin. While newer agents offer promise for dealing with multi-resistant organisms in the region, there remains a need for an affordable oral agent which can reliably treat MRSA, as well as the relevant Gram-negative pathogens. This would allow outpatient treatment, where possible. Delafloxacin, which was approved in 2017 by the US Food and Drug Administration (FDA) for acute bacterial skin and skin structure infections (ABSSSIs), offers these advantages [59,60], but is not currently licensed in the 5 Gulf countries (Bahrain, Kuwait, UAE, Oman, and Qatar). The rise of multidrug-resistant pathogens, and frequency of adverse events have led to restricted use of the preferred antibiotics which are taken orally, such as fluoroquinolone, cephalosporins, or amoxiclav [61,62]. The availability of treatment in a region and overcall cost-effectiveness of treatment must also be factored into treatment decisions.
Ceftaroline, recently introduced in the 5 Gulf countries, is an advanced 5th generation cephalosporin that has been approved for use against CA-pneumonia and cSSTI.
Ceftaroline possesses bactericidal activity against Gram-positive bacteria, including MRSA, and Gram-negative bacteria [63]. With respect to susceptibility data, studies in African and Middle Eastern countries showed that all methicillin-susceptible S. aureus and 91.8% of MRSA were susceptible to ceftaroline, and the rates of susceptibility to ceftaroline amongst extended-spectrum beta-lactamase (ESBL)-negative Escherichia coli, Klebsiella pneumoniae and K. oxytoca ranged from 89.1% to 99.0%, respectively [64].
Ceftobiprole is another 5th-generation cephalosporin that is currently available in Saudi Arabia and is expected to be available in 5 Gulf countries in the near future. Ceftobiprole also possesses broad bactericidal activity against Gram-positive bacteria, including MRSA, and Gram-negative bacteria, such as Pseudomonas [65]. While currently approved for the treatment of adults with CA- or HA-pneumonia (excluding ventilator associated pneumonia) by the European Medicines Agency (EMA), it is yet to receive approval for use against cSSTIs.
1.7. Diagnostic and therapeutic pathway in patients with cSSTIs
A clear diagnostic and therapeutic pathway is a crucial part of the patient diagnostic process. This should span everything from the initial Emergency Department admission through diagnosis and treatment, until hospital discharge. A multidisciplinary approach based on clear hospital-based guidelines is recommended, including diagnostic testing ahead of surgery, referring the patient to an appropriate team of specialists including the surgeon, clinical pharmacist, clinical microbiologist, intensivist, and infectious disease specialist. In the cases of severe infections, the treatment decision could take place prior to diagnosis, and if empirical therapy is used, it should focus on patient profile, as well as the local epidemiology of cSSTIs.
1.8. Treatment stratification principles
There is a tendency to overuse or misuse antibiotics in the Gulf Cooperation Council countries (Bahrain, Kuwait, UAE, Oman, Qatar, and Saudi Arabia) [66], adding to the already existing challenge of antimicrobial resistance within these regions. For optimal management of patients with cSSTI, stratifying patients based on their individual risk factors; causative organisms and available treatment options are strongly recommended [44]. In hemodynamically stable patients, the necessity for surgical source control (e.g., abscess) or conservative treatment (e.g., erysipelas) needs to be evaluated 1st by an interdisciplinary team led by an experienced surgeon. In mild infections, surgical drainage alone is usually sufficient for patients without risk factors or significant comorbidity. Patients with risk factors such as diabetes or immunosuppression may require oral antimicrobial treatment in addition to surgical source control, even in mild infections.
Severe infections are characterized by failure of oral antimicrobial treatment, failure of incision and drainage, systemic signs of infection, an immunocompromised state, and clinical signs of deeper infections or evidence of organ dysfunction [5]. These patients usually require hospitalization, intravenous antimicrobial treatment, and/or intensified surgical source control. In severe infections, an antimicrobial treatment is recommended regardless of coexisting risk factors. Patients with sepsis or septic shock require immediate care [67,68]; surgical intervention, hemodynamic stabilization, and a broad intravenous antimicrobial choice within an hour of admission to hospital.
2. Antimicrobial treatment of cSSTIs in Bahrain, Kuwait, UAE, Oman, and Qatar in an era of multidrug-resistant pathogens
The most commonly observed cSSTIs in the 5 Gulf countries studied are the major cutaneous abscesses, erysipelas, surgical-site infections, cellulitis, infected ischemic ulcers/infected venous stasis ulcers, and infected decubitus ulcers. These cSSTIs along with their causative pathogens, primary disciplines involved in its management, surgical treatment options, and available antimicrobial substances are presented in Table 4. The high prevalence of MRSA in almost all Gulf countries calls for a specific approach in patients known or suspected to be infected with MRSA. Patients with mild-to-moderate infections tend to have few risk factors and present with localized infections (e.g., small abscesses due to CA-MRSA) which require only incision and drainage (no antibiotics are necessary). Those with risk factors and/or significant comorbidity can be generally treated with orally available substances.
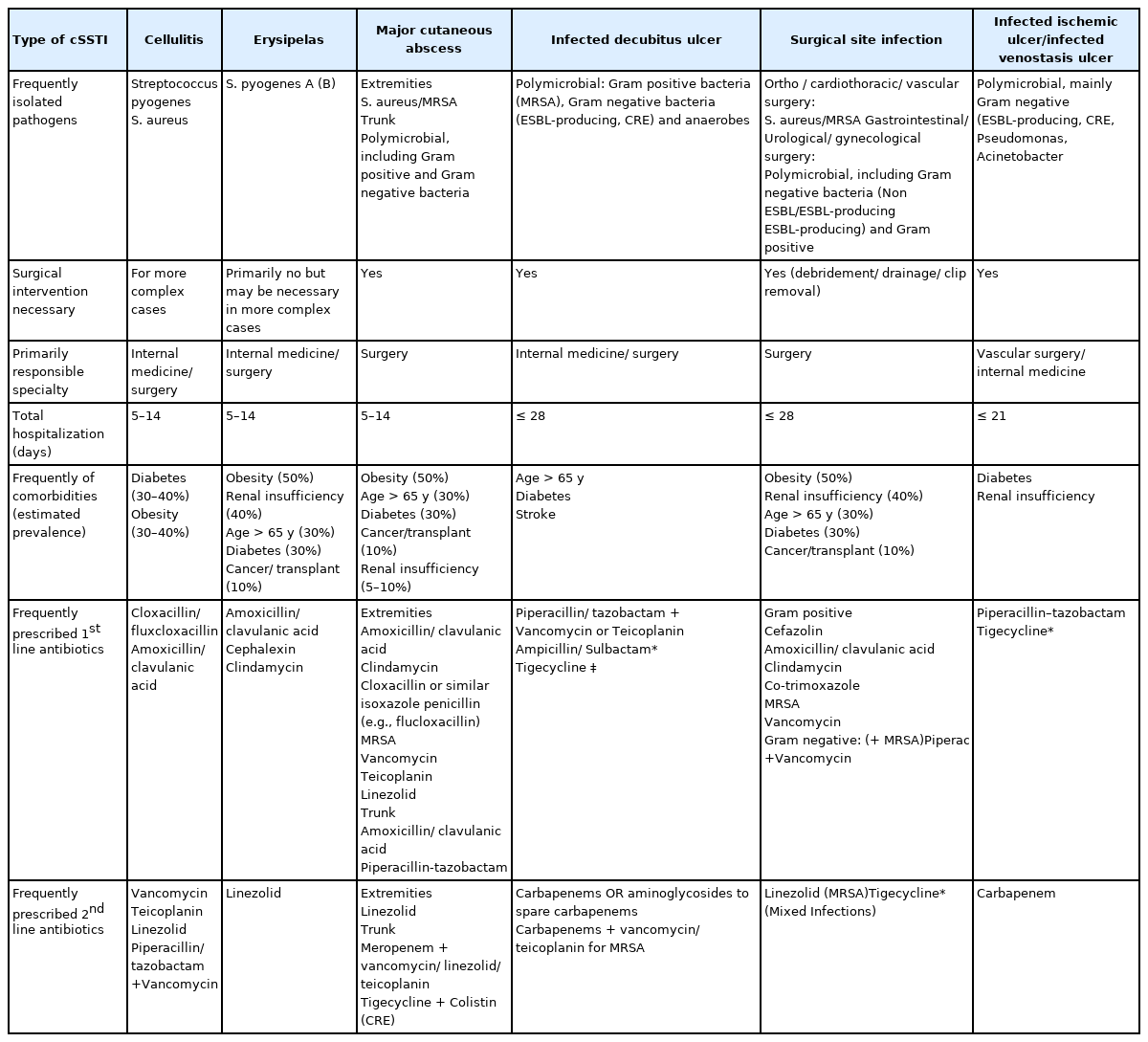
Frequent cSSTIs in the Gulf and current treatment pathways.
For patients with severe infections, intravenous antimicrobial treatment is generally recommended. Clinicians should determine the likelihood of; (1) a monomicrobial MRSA infection (e.g. an extended abscess of an extremity); or (2) a polymicrobial infection including MRSA, and susceptible Gram-negative organisms (e.g. perineal abscess in a patient known to be colonized with MRSA); or (3) a polymicrobial infection with the involvement of resistant Gram-positive (MRSA) and Gram-negative (ESBL-producing or Carbapenem-resistant enterobacterales) pathogens (e.g. necrotizing fasciitis in a multimorbid patient with multiple recent hospitalizations). Tigecycline is an option in hemodynamically stable patients, even in elderly patients [69], but it should not be used as a monotherapy in septic shock. Vancomycin use is not recommended in patients with impaired renal function. The initial antimicrobial therapy should be aligned to the latest isolated organisms, most frequently in terms of de-escalation. A switch to oral therapy is possible if the clinical criteria for oral antibiotic treatment are fulfilled [70]. Nevertheless, adherence to oral antibiotic treatment in cSSTIs is often jeopardized by reduced compliance rates [71]. Empirical treatment regimens frequently used in the treatment of MRSA cSSTI under different bacterial etiology and clinical conditions, their limitations, available alternatives, and common toxicities associated with the antibiotic of choice are shown in Table 5 [2,72–80].
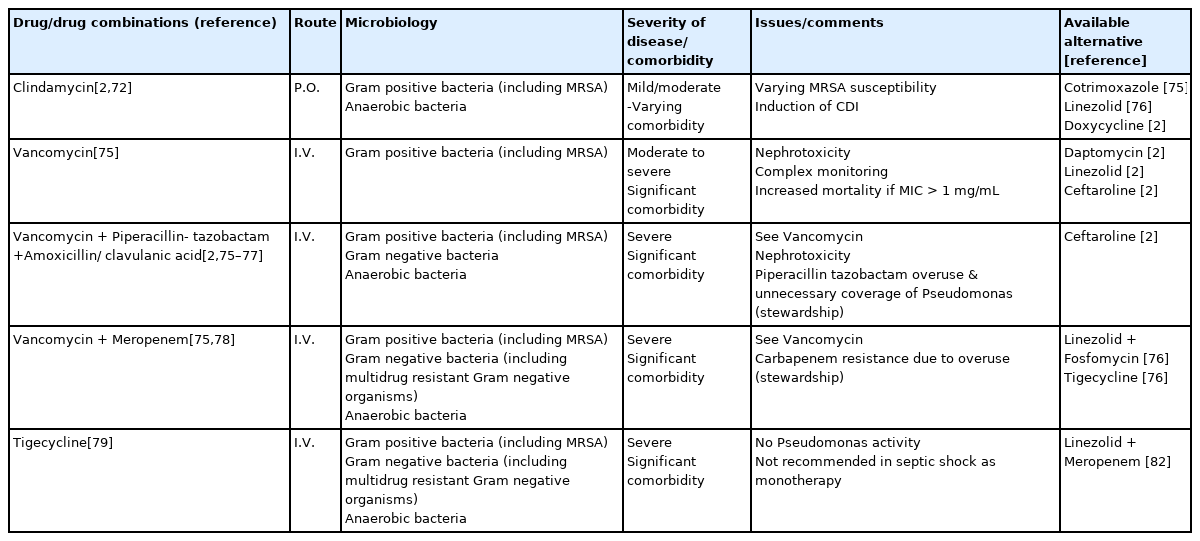
Empirical treatment of MRSA in cSSTIs in 5 Gulf countries: Clinical conditions, limitations, and available alternatives.
2.1. Duration of antimicrobial therapy
Many mild-to-moderate infections require only surgical source control, meaning that use of antibiotics can be spared. In general, antibiotic treatment courses in cSSTI requiring surgical intervention, should be short. The standard antibiotic treatment duration for mild infections is 5–7 days, which can be extended to 7–10 days in severe infections, especially in critically ill patients [2]. There is no evidence supporting a long-term duration of antibiotics in any cSSTI. Effort must be made to reduce the duration of patient treatment in order to protect patients from the potentially toxic side effects of antibiotics, and the development of antimicrobial resistance, as well as reduction of the costs associated with unnecessary extended use of antimicrobials in the treatment of cSSTIs [81]. An evaluation of the patient’s condition, and laboratory cell culture results within 72 hours of admission to hospital can direct clinicians to switch from intravenous to oral treatment, consider outpatient parenteral antibiotic therapy, de-escalate treatment to a narrower spectrum agent, or even guide a decision towards the need for surgery, or to discharge the patient [70].
2.2. Preconditions for successful guideline implementation
Due to limited national guidance for the everyday clinical management of cSSTIs, of the 5 Gulf countries, rely on local hospital guidelines or international guidelines. This highlights the need for a more comprehensive approach to the clinical management of cSSTIs and greater alignment on the guidelines across the 5 Gulf countries studied. Using clear, recognized classification systems, particularly for describing disease severity and assessment, these should clarify the position of novel agents in the treatment paradigm. Recognized staging/ scoring systems should be used for patient diagnosis and stratification, which should be based on the local patient population and their risk factors, and the importance of infection source control must underpin the management of all cSSTIs [82]. Management strategies must include steps to swiftly identify which cases require immediate medical or surgical attention and intervention, and treatment options should be based on patient need, classification of infection (HA-MRSA or CA-MRSA) if relevant, along with the availability of resources. A specific sepsis protocol should be included in cSSTIs guidance, ideally recommending that patients receive antibiotics within an hour, instead of waiting for cell culture results. The roles and responsibilities of healthcare professionals must be clearly defined at each stage of patient management. If prescribing is restricted to individuals (for example, infectious disease specialists), this must be clearly communicated in order to prevent treatment delay.
Crucially, recommendations must encourage antimicrobial stewardship in both inpatient and outpatient settings, involving all healthcare professionals in the treatment pathway of a patient, including guidance for general practitioners and family physicians. This information in the guidelines should be used by the entire multidisciplinary team involved in managing cSSTIs, including infectious disease specialists, clinical microbiologists, Emergency Department healthcare providers, intensive care physicians, infectious disease physicians, and surgeons. Treatment can then be optimized and standardized whilst maintaining antimicrobial stewardship standards. For example, by electing simple surgery to avoid the overuse of oral antibiotics, or by relaxing restrictions on certain antibiotics in pre-specified cases, such as those with sepsis.
Conclusion
To tackle the rise of multi-antibiotic resistant bacteria, and remove barriers to optimize treatment in Bahrain, Kuwait, UAE, Oman, and Qatar, the management and treatment of cSSTIs needs to be reconsidered with special attention to the following areas:
Application of an inclusive definition of cSSTIs which aligns with clinical and research purposes.
Collection of comprehensive up-to date epidemiological data on cSSTIs and MRSA in a region, using local and regional registries, financed by centralized and regional health authorities.
Clear indications in place for the use of novel agents and a comprehensive assessment of comparative agents to be factored into the decision-making for treatment of cSSTIs.
Guidance for the management of patients with cSSTI which is applicable to Bahrain, Kuwait, UAE, Oman, and Qatar.
Improved access and availability to rapid diagnostics and treatments for MRSA from a cost perspective and a patient need perspective.
Improved education and awareness of cSSTIs and their management among newly qualified physicians, those in training, and primary care physicians is essential.
Antimicrobial stewardship initiatives to reduce the inappropriate use of antibiotics and aid judicious use and appropriate duration of use of antibiotics.
cSSTIs comprise multifaceted infections and present numerous challenges for patients and those who care for them. We present our recommendation hoping that this collaborative guidance will help clinicians optimize the management and treatment of cSSTIs in patients across Bahrain, Kuwait, UAE, Oman, and Qatar, and reduce the burden on the local healthcare system.
Acknowledgments
The authors of this review convened an expert panel in a sponsored meeting and were not appointed by national societies or regulatory authorities in the respective countries. Medical writing and editorial assistance were provided by Aisling Koning and Kyle Lambe (Synergy Medical Communications, London, UK), and was supported by Pfizer, Inc. Additional editorial support was provided by Vaidehi Wadhwa (Center of Excellence, Emerging Markets, Pfizer).
Notes
Conflicts of Interest
Wadha Alfouzan reports payment for advisory board meetings, presentation and research funding from Pfizer, Inc., MSD, and Sanofi. Nervana Habashy reports employment from Pfizer, Inc. Ayman Kurdi reports employment and stock ownership from Pfizer, Inc. Christian Eckmann reports personal fees from Pfizer, Inc. during the conduct of the study; and personal fees from Menarini, Nabriva and Pfizer, Inc. outside the submitted work. All other authors report no potential conflicts of interest.
Ethical Statement
This research did not involve any human or animal experiment.