Clinical Outcomes of Emergent Laparotomies in Hypotensive Patients: 9-years Experience at a Single Level 1 Trauma Center
Article information

Abstract
Purpose
The prognosis of an emergent laparotomy in hypotensive patients is poor. This study aimed to review the outcomes of hypotensive patients who had emergent laparotomies and elucidate the risk factors of mortality.
Methods
Patients who underwent an emergent laparotomy from January 2011 to December 2019 were retrospectively reviewed. The exclusion criteria included initial systolic blood pressure > 90 mmHg, aged < 19 years, and cardiac arrest before the laparotomy. Patients were categorized into survival groups (survived or deceased). Univariate and multivariate analyses were conducted to determine the risk factors of mortality. The time from the laparotomy to death was also reviewed and the effect of organ injury.
Results
There were 151 patient records, analyzed 106 survivors, and 45 deceased. The overall mortality was 29.8%. Liver injury was the main organ-related event leading to an emergent laparotomy, and most patients died in the early phase following the laparotomy. Following multivariate analysis, the Glasgow Coma Scale score [odds ratio (95% confidential interval) 0.733 (0.586–0.917), p = 0.007], total red blood cell transfusion volume in 24 hours[1.111 (1.049–1.176), p < 0.001], major bleed from the liver [3.931 (1.203–12.850), p = 0.023], and blood lactate [1.173 (1.009–1.362), p = 0.037] were identified as risk factors for mortality.
Conclusion
Glasgow Coma Scale score, total red blood cell transfusion volume in 24 hours, major bleed from the liver, and lactate were identified as risk factors for mortality. Initial resuscitation and management of liver injuries have major importance following trauma.
Introduction
Hemorrhagic shock is the most common cause of preventable death following trauma [1]. Abdominal injuries can result in a major bleed, which often indicates the necessity for an emergent laparotomy. However, the extent of mortality after this procedure is serious [2]. In 2002, a multicenter cohort study conducted in the United States reported that the mortality rate for hypotensive trauma patients undergoing emergent laparotomies was approximately 40% [3]. In 2017, another multicenter cohort study from the United States reported the mortality rate of emergent laparotomies to be 21%. However, the mortality rate for hypotensive patients appeared unchanged at 46%, despite improvements in trauma care [4].
In the Republic of Korea in 2012, the government implemented the use of regional trauma centers. Since trauma patients are directed to a regional trauma center, it is easier to collect patient data, and the time taken to start an emergent laparotomy is monitored in hypotensive patients.
Recent studies from 1 of these trauma centers have reported that mortality after damage control surgery was about 42% [5,6], which was similar to studies in the USA [3,4]. Mun et al also reported that mortality after a trauma laparotomy in major trauma patients was 23.7% [7]. Ajou University Medical Center, Suwon, Korea currently acts as a regional trauma center, enabling the collection of patient data using the Korean Trauma Data Bank. The purpose of this study was to review the outcome of patients with hypotensive trauma who had an emergent laparotomy and to elucidate the risk factors associated with mortality.
Materials and Methods
This study was reviewed and approved by the appropriate institutional review board (no.: AJIRB-MED-MDB-20–581). This study included trauma patients who underwent an emergent laparotomy from January 2011 to December 2019. The exclusion criteria were as follows: initial systolic blood pressure (SBP) > 90 mmHg, aged < 19 years, and cardiac arrest before laparotomy. The patients included in this retrospective review were categorized into 2 groups according to whether they survived or deceased. Patient data regarding their initial physiological parameters, general characteristics, injury severity, and treatment was also collected. Injury-to-operation time was defined as “the time from injury to the first surgical incision,” and operation duration was defined as “the time from the first surgical incision to closure” (including temporary closure).
Comparisons between the groups were performed using the Student t test or the Mann-Whitney U test (after normality tests for continuous variables). Variables were presented as mean ± standard deviation for the Student t test, and as the median (interquartile) for the Mann-Whitney U test. The Chi-square test or the Fisher’s exact test was used for categorical variables. Following univariate analysis, variables with p < 0.05 were included in the multivariate analysis by applying binary logistic regression. The results of the binary logistic analyses were summarized by estimating the odds ratios and the respective 95% confidence intervals. All analyses were performed using IBM SPSS Version 21.0 (IBM Corp., Armonk, NY, USA).
Results
1. Patient characteristics
Amongst the 908 patients who underwent an emergent laparotomy, there were 151 patients who were included in the analysis. Of these, 106 patients survived and 45 died. The overall mortality rate was 29.8% (Figure 1). Overall, the Trauma and Injury Severity Score was 61.5%. Amongst the 45 deceased patients, 19 (42.2%) died due to a hemorrhage (all within 24 hours of surgery), 20 (44.4%) died from organ failure, and 6 (13.3%) died from severe brain damage. Compared with the group that survived, the deceased group displayed a lower SBP (75.1 ± 13.0 vs 63.5 ± 20.0, p < 0.001), a lower Glasgow Coma Scale (GCS) score (11.7 ± 3.9 vs 6.0 ± 4.5, p < 0.001), and a higher lactate level (5.2 ± 3.3 vs 8.5 ± 3.8, p < 0.001; Table 1).

Flowchart of study inclusion.
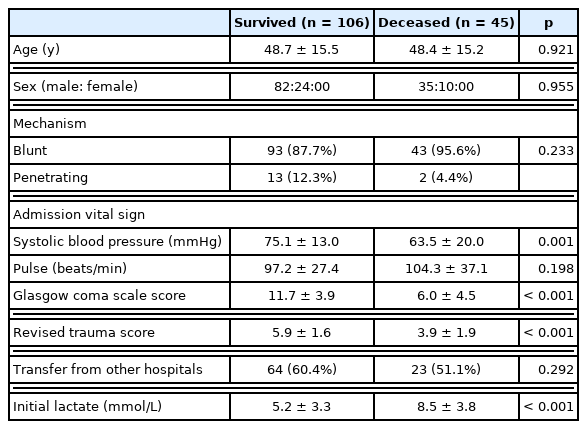
General patients’ characteristics on admission.
2. Injury severity and outcome of laparotomy
Using the Abbreviated Injury Scale (AIS), the liver was the most common major organ injury, and was also considered the most life-threatening factor. Amongst hypotensive patients with a major bleed from the liver, 55.3% of patients died. No mortality was observed in those with injuries to the pancreas, colon, abdominal wall, or bladder (Figure 2).

Mortality according to the highest Organ Injury Scale scores.
* Other: Duodenum, bladder, rectum, and abdominal wall.
† Multifocal: Injuries of the highest grade for more than 2 organs.
SMA = superior mesenteric artery; SMV = superior mesenteric vein.
The deceased group experienced more severe injuries and required higher volumes of transfused red blood cells (RBC), however, there was no significant difference in the time from injury to operation or admission to operation (Table 2) between the groups. Most patients in the deceased group died within 24 hours (Figure 3A). There were 19 patients who died due to a hemorrhage, 2 patients died from organ failure, and 1 patient died from severe brain damage. Of those who died within 24 hours of surgery, 9 (40.9%) patients died within 1 hour of the operation (Figure 3B).
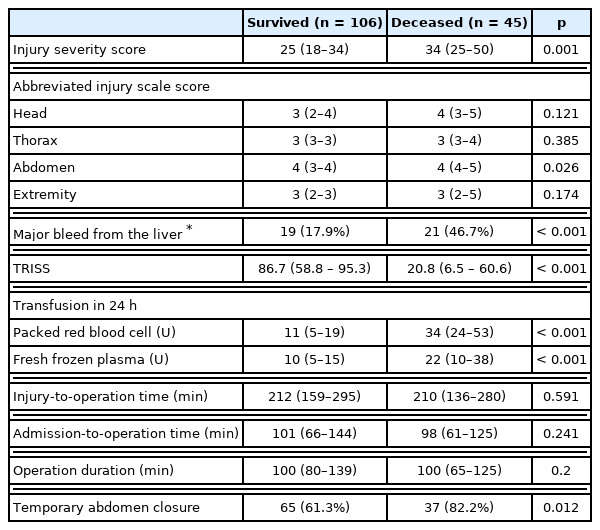
Injury characteristics of laparotomy.

Timing of death (A) days after admission following a laparotomy; (B) hours within the first day.
3. Risk factors of mortality after laparotomy in hypotensive patients
Univariate analysis was applied to the GCS score, Revised Trauma Score, Injury Severity Score, a major bleed from the liver, total RBC and fresh frozen plasma (FFP) transfusion volumes within 24 hours, lactate levels, and the percentage undergoing temporary abdomen closure were all selected for multivariable analysis. Following multivariate analysis, the GCS score [odds ratio (95% confidence interval): 0.733 (0.586–0.917), p = 0.007], total RBC transfusion volume in 24 hours [1.111 (1.049–1.176), p < 0.001], major bleeding from liver [3.931 (1.203–12.850), p = 0.023], and elevated blood lactate [1.173 (1.009–1.362), p = 0.037] demonstrated significant differences between the survived and deceased groups (Table 3).
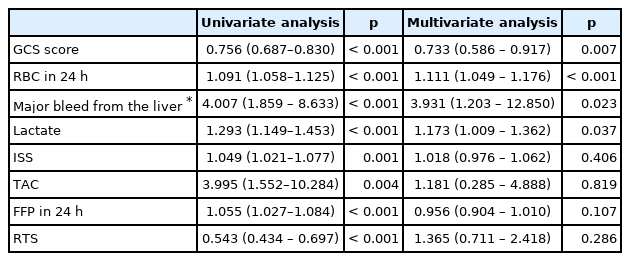
Univariate and multivariate analyses for risk factors of mortality.
Discussion
Emergent laparotomies in hypotensive patients following trauma is associated with a high mortality rate. Understanding the risk factors associated with mortality, which are yet to be fully elucidated, is of the utmost importance. In this retrospective study, the overall mortality of 29.8% was lower than the rates observed in previous studies in the USA [3,4], and Korea [5] (40–46%)
Among the deceased group, more than half of the patients died within a day after the laparotomy, and most of these deaths occurred within 5 hours. Hemorrhages are the leading cause of death following trauma, so emphasis is on early hemorrhagic control [5,8]. However, the debate as to whether time to laparotomy is an important factor for survival is ongoing. Barbosa et al demonstrated that an increased time to operation was associated with mortality in face, arm, speech test positive patients [9]. In contrast, Undurraga Perl et al [10] reported that the resuscitation strategy, including time to laparotomy, did not affect survival. Similarly, Groven et al [11] reported that an increased time to laparotomy did not increase mortality. In the current study, a difference in time to laparotomy between the survival and deceased groups was not observed. However, unlike other studies where the time to a laparotomy was around 30–40 minutes, in this current study approximately 100 minutes elapsed between admission and the operation. The implementation of regional trauma centers began in 2012 in Republic of Korea, and the trauma center in Ajou University Medical Center, Suwon, Korea was built 2016. It seemed that the trauma system of care had been slow to be adopted in Korea compared with other countries. Clarke et al [3] demonstrated that the time to a laparotomy did affect survival, but only for delays up to 90 minutes. Therefore, the time to a laparotomy in the current study was possibly too long (100 minutes) to impact survival, and an increased effort to shorten this time is required.
This current study did reveal a significant difference in the GCS score between the surviving and deceased groups. The GCS score is a well-known predictor of survival in patients with head trauma and overall trauma [12,13]. Moreover, it can be used as a predictor of mortality in patients with pelvic trauma or for those patients who undergo damage-control laparotomy [14,15]. Consistent with these studies, following multivariate analysis, the results of this study showed that a statistically lower GCS score was a risk factor of mortality between the 2 groups, despite there being no statistical difference observed in the AIS score for the head. The GCS score reflects cerebral perfusion, which could potentially be reduced by hemorrhagic shock. Therefore, the GCS may be a stronger predictor of the probability of survival than SBP, respiratory rate, and even the Injury Severity Score [16,17].
The amount of blood transfusion required for a patient is related to the extent of bleeding, therefore, the total RBC transfusion volume in 24 hours was also a risk factor in the current study. However, the amount of FFP transfused in 24 hours was not a risk factor following multivariate analysis. In addition to the total transfusion volume (the FFP to RBC transfusion ratio) was also important in trauma patients who received massive blood transfusion. Roquet et al demonstrated that an FFP:RBC ratio of more than 1:1.5, transfused within 6 hours, improved the 30-day mortality rate in trauma patients with severe bleeding [18]. Although the FFP to RBC ratio was not specifically reviewed in this study, the ratio was higher in the survival group, at almost 1:1 compared with 1:1.5 in the deceased group.
Regarding the effects of organ injury, even when using the same injury scale, the rate of mortality is different depending on the damaged organ. Damage to the liver shows the poorest outcome among Grade IV–V injuries [19]. Similarly, in this current study, more than half of the patients with a major bleed in the liver had deceased. Management of severe liver injuries is challenging but has improved with the adoption of a multidisciplinary approach [20,21]. Grade IV–V injuries to the pancreas or colon have been associated with a mortality rate of 28–32% [19], however, in the current study in patients with injuries to the pancreas and colon no mortality occurred. This may be because the number of patients with pancreas and colon injuries was small and the highest injury grade was Grade III.
This study had several limitations. Firstly, the study design was retrospective, and the number of patients was too small for meaningful epidemiological analysis. Secondly, during the 9-year study period, trauma care has improved through the implementation of trauma centers within hospitals. Thirdly, main abdomen organ injury was presented in this study but multiple lower grade abdomen organ injuries were excluded from analysis. In conclusion, emergent laparotomies in hypotensive patients resulted in a high mortality rate. The GCS score, total RBC transfusion volume in 24 hours, a major bleed from the liver, and blood lactate were determined to be significant risk factors for mortality. Furthermore, mortality mostly occurred within 24 hours of the laparotomy, hence, early control of bleeding is important and could reduce the total RBC transfusion, which is a risk factor of mortality. Management of liver injuries remains a challenge in trauma laparotomy.
Notes
Conflicts of Interest
The authors declare no conflicts of interest to declare.