Assessing Clinical Feasibility and Safety of Percutaneous Dilatational Tracheostomy During Extracorporeal Membrane Oxygenation Support in the Intensive Care Unit
Article information

Abstract
Purpose
A tracheostomy is often used to wean patients off the ventilator, as it helps maintain extracorporeal membrane oxygenation (ECMO) without sedation. A percutaneous dilatational tracheostomy (PDT) performed in critically ill patients is widely accepted, however, its feasibility and safety in ECMO is unclear.
Methods
This retrospective observational study included 78 patients who underwent a PDT and ECMO at the surgical intensive care unit (SICU) in a tertiary hospital between January 1, 2016 and December 31, 2019. We analyzed their medical records, including PDT-related complications and clinical variables.
Results
The median values of hemoglobin, platelet count, international normalized ratio, partial thromboplastin time, and activated partial thromboplastin time before the tracheostomy were 9.2 (8.5–10.2) g/dL, 81 (56–103) × 103/dL, 1.22 (1.13–1.30), 15.2 (14.3–16.1) seconds, and 55.1 (47.4–61.1) seconds, respectively. No clotting was observed within the extracorporeal circuit, however, minimal bleeding was observed at the tracheostomy site in 10 (12.8%) patients. Of 4 patients with major bleeding, local hemorrhage was controlled in 3 patients, and intratracheal bleeding continued in 1 patient. The mortality rate was 60.9% and 57.1% in the complication and no-complication group, respectively. The durations of SICU stay, hospital stay, and mechanical ventilation were not statistically different between the groups.
Conclusion
A PDT performed in critically ill patients was associated with a low rate of bleeding. Complications did not appear to significantly affect the patient outcome. PDT can be performed in patients who usually require a tracheostomy to maintain ECMO.
Introduction
Currently, extracorporeal membrane oxygenation (ECMO) serves as a support for patients with respiratory disorders, including various forms of severe hypoxic or hypercapnic respiratory failure [1]. Most patients on ECMO are administered sedation with mechanical ventilation (MV) [2]. Patients on ECMO often receive prolonged MV, which may result in increased requirement for sedation [3]. Increased sedation can lead to low blood pressure, venous thrombosis, increased risk of long-term ventilation, and increased risk of pneumonia in patients, and an increased workload on the staff, increased bed occupancy, and related costs [4]. Unfortunately, prolonged endotracheal intubation is not an appropriate solution either because it increases the risk of pneumonia, tracheal necrosis, sedation requirements, and an extended stay in the intensive care unit (ICU). Therefore, in the ICU, for most patients on ECMO who are administered sedation and MV there may be an increase in immobility and use of vasoactive drugs, and total intravenous fluids, as well as other relevant sedation-related adverse effects. To overcome these problems, a tracheostomy for patients who are stabilized with ECMO may be considered. A tracheostomy is performed in the ICU to expedite the weaning off from MV in addition to restoring upper airway function, improving tracheobronchial toileting, and decreasing the chance of injury to the vocal cords [5,6]. Recently, performing a percutaneous dilatational tracheostomy (PDT) in a critically ill patient has gained widespread acceptance as a management strategy [7]. A PDT is performed using the Seldinger technique, which was first described by Shelden and Pudenz in 1957 [8]. Given the relative simplicity and pace at which this procedure is available and can be performed at the bedside, the PDT has become quite popular and has replaced surgical tracheostomies (ST) in many ICUs [7]. Nevertheless, the use of the PDT as a procedure of choice is still limited in patients on ECMO, which could be due to the perception by surgeons that the PDT is not beneficial or is associated with an increased risk of bleeding. Therefore, the aim of this study was to evaluate the feasibility and safety of the PDT in patients on ECMO.
Materials and Methods
Patients who underwent a PDT while on ECMO support at a tertiary hospital in South Korea between January 1, 2016 and December 31, 2019 were retrospectively reviewed. The Ciaglia Blue Rhino kit (Cook Critical Care, Bloomington, IN, USA) was used for the PDT procedure. This kit includes a curved dilator such that the nose of the rhino is inserted over a guiding catheter and creates a tracheostomy opening. ECMO was administered according to the general treatment principles, and heparin was administered based on each patient’s conditions. Additionally, the timing of the PDT was determined by the intensivist and attending physician, based on the patient’s condition, and the possibility of weaning. The following clinical baseline data were routinely collected: age, sex, primary diagnosis, hospital and ICU durations of stay, mortality, type of ECMO support, number of days in ICU prior to ECMO, duration of ECMO and MV, duration between initiating MV and ECMO support, duration between ECMO and PDT, complications of PDT, blood transfusions, and anticoagulation. Additionally, the following hematological and coagulator parameters were assessed: pre-PDT and post-PDT hemoglobin levels, platelet count, international normalized ratio (INR), partial thromboplastin time (PT), and activated partial thromboplastin time (aPTT) prior to the PDT.
Statistical analysis was performed to classify patients based on complications and in order to compare clinical variables including mortality, laboratory data, use of heparin, durations of ICU and hospital stay, and MV duration between the groups. Continuous variables were expressed as the median and interquartile range. Categorical variables were expressed as a count and percentage. Depending on the number of groups compared and the data type, Chi square test, Fisher’s exact test, or Mann-Whitney test were used. A 2-sided p < 0.05 was considered significant. SPSS Version 20.0 (SPSS Inc., Armonk, NY, USA) was used to perform the analyses. The ethics committees of Hallym University Institutional Review Board approved this study, and the requirement for informed consent was waived due to the retrospective study design.
Results
1. Baseline characteristics
There were a total of 270 patients who received ECMO. Among these patients, 78 underwent a PDT (no other tracheostomy technique was used). The overall median age was 59 years (range, 26–62.5), and 61 patients (78.2%) were men. A total of 28 patients (35.9%) were on veno-venous (VV) ECMO, and 50 patients (64.1%) were on veno-arterial (VA) ECMO. The main causes for performing ECMO were pneumonia (n = 22), and acute myocardial infarction (n = 21; Table 1) At the time of the PDT, 26 patients were administered heparin, while the other patients were supported with ECMO without anticoagulation due to bleeding complications before the PDT (Table 1). The median duration until the PDT was 5 days (4–8) after intubation, and 5 days (3.25–7) after ECMO initiation. An early tracheotomy (< 8 days after intubation) was performed in 55 patients (70.5%). The median values for preprocedural hemoglobin, platelet count, INR, PT, and aPTT before PDT were 9.2 (8.5–10.2) g/dL, 81 (56–103) ×103/dL, 1.22 (1.13–1.30), 15.2 (14.3–16.1) seconds, and 55.1 (47.4–61.1) seconds, respectively. The median level of hemoglobin in the 24 hours following the PDT was 9.2 (8.6–10.1) g/dL, which was similar to that during the previous 24 hours (Table 1).

Baseline clinical characteristics of patients with PDT on ECMO (January 1, 2016 to December 31, 2019).
2. Incidence of bleeding complications
There were no PDT procedure-related deaths or periprocedural thrombotic complications related to ECMO. There were noticeable bleeding complications in 4 patients. Three patients developed bleeding at the tracheotomy site which required electrocauterization. Another patient had continuous intratracheal bleeding for 48 hours following the PDT. All 4 patients were undergoing VV ECMO at the time of the PDT. Other complications were classified as minor bleeding (n = 10, 12.8%) and required simple observation (Table 2). All patients with bleeding were hemodynamically stable and no transfusions were performed. Additionally, there was no statistically significant difference between the complication and no-complication groups in terms of the laboratory findings and other clinical data (Table 3). Overall, 26 of 78 patients were administered anticoagulation therapy with heparin during the PDT (Table 1). Regarding the incidence of major or minor bleeding, there was no significant difference between the group of patients who received heparin and the group who did not (p = 0.261; Table 3).
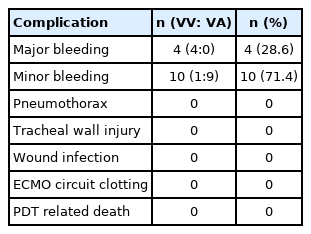
PDT related complications.
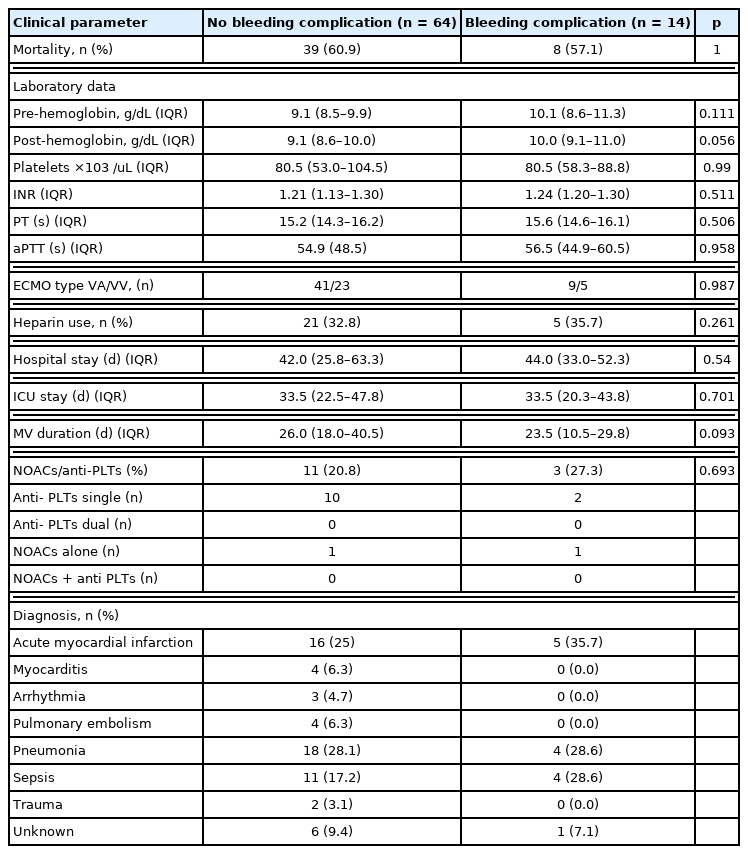
Clinical data comparing patients with and without bleeding complications.
3. Clinical course and outcomes
The total mortality rate was 60.3% (n = 47). The most common cause of mortality was septic shock (n = 37; Table 4). The rates for weaning off ECMO and ventilation were 61.5%, and 44.9%, respectively (Table 1). There were no significant differences in the mortality rates between the complication and no-complication groups (62.5% vs. 57.1%, respectively; p = 0.767). Additionally, the median durations of hospital and ICU stays were not significantly different between groups (Table 3). The total MV duration, ECMO support, and ICU/hospital duration are presented in Table 1.

All cause of mortality of ECMO patients.
Discussion
The use of the PDT in patients on ECMO did not have a significant effect on the outcome of the critically ill patients in this study. Additionally, it was determined that the frequency of complications was low and the incidence of complications did not affect the outcome.
Recently, the awareness of the potential usefulness of early mobilization and rehabilitation of patients on ECMO has increased [9,10]. For this purpose, many clinical centers opt to use a tracheostomy in these patients [11]. Although tracheotomies are an invasive procedure, it has been reported that this procedure offers various advantages over traditional translaryngeal intubation, such as a reduced risk of inadvertent extubation, decreased physical and psychological discomfort, increased MV weaning rates, and a lower risk of ventilator-associated pneumonia [12]. Additionally, the tracheostomy has several other clinical benefits, including early initiation of physical therapy and active rehabilitation, facilitating pulmonary toilet, and intermittent MV to help prevent lung collapse, especially in patients with fatigue following active rehabilitation [13,14]. However, several centers do not permit tracheostomies during ECMO due to the increased risk of bleeding [15]. In fact, ECMO causes coagulopathy and thrombocytopenia through several mechanisms [16]. An ECMO circuit consists of a mechanical blood pump, a gas exchange device (membrane oxygenator), and a heat exchange device connected together with circuit tubing [17] and blood is constantly in contact with these surfaces, which results in a prothrombotic state. Therefore, the ECMO circuit elicits a prothrombotic response, which can lead to consumptive coagulopathy as a result of activation of clotting factors, and excessive fibrinolysis [18,19]. Consumptive coagulopathy causes bleeding or a tendency to bleed, and widespread intravascular thrombotic obstruction of vessels, which are attributed to multi-organ failure. In this current study, the average platelet, INR, PT, and aPTT levels in these patients were all lower than their respective normal range (Table 1). Generally, there is an increased risk of bleeding in this group when anticoagulation is required to reduce clotting within the ECMO circuit [20]. However, a previous study reported no correlation between thrombocytopenia and bleeding risk [21]. This result was similar to what had been observed in several other studies, which reported that thrombocytopenia was not an independent risk factor for bleeding after a tracheostomy [21,22]. It was determined in this current study that administration or non-administration of heparin was not related to bleeding complications (Table 1). A recent study has demonstrated that heparin-free ECMO is being used in specific patient groups, such as those with trauma [23]. In addition, membranes of the ECMO circuit that do not require anticoagulation are being developed [24]. Therefore, the level of concern about coagulopathy in patients on ECMO, which were raised in the past, appear to be gradually decreasing. This paves the way for bolder invasive procedures, for patients on ECMO.
In this current study, there were 14 patients on ECMO (17.9%) who underwent a tracheostomy and developed bleeding at those sites. However, only 4 (5.1%) had noticeable bleeding and required additional procedures. In the remaining 10 patients, only minor bleeding (oozing) was observed and the bleeding stopped spontaneously without further treatment. There was no statistical significance between the use of heparin and complications (p = 0.261). Additionally, pneumothorax, wound infection, and tracheal injury were not observed in this current study and there was no circuit change necessary due to clotting (Table 2). Previous studies and results from this current study suggest that tracheostomies in patients on ECMO are generally feasible when it is not accompanied by severe coagulopathy [25]. In the past, a tracheotomy was implemented with complex open technical techniques, however, since the development of the PDT technique which is cost-effective, simple, and rapid, it is commonly used. Additionally, the use of the PDT is increasing in the ICU [26]. In particular, the PDT can be performed more safely and accurately using bronchoscopy. Several studies have reported that there is no significant difference between the complication rates arising from a PDT compared with performing a ST, although more wound complications occur during a ST [27–29]. However, the major challenge of bleeding during the tracheostomy procedure is hemostasis. Therefore, the indications along with the risks and benefits of a tracheostomy should be carefully examined on an individual basis. Owing to the nature of the PDT procedure, blind access is surgically created through the skin of the neck to the trachea. Therefore, using this access it is difficult to identify the focus of bleeding, if bleeding occurs at this site, or if the surrounding blood vessels are injured. Further operations may be required for hemostasis, therefore, until recently, the application of the PDT was considered difficult in patients with coagulopathy. Coagulopathy by itself is not considered a contraindication to PDT, however, if bleeding occurs during the procedure coagulopathy may interfere with hemostasis. Therefore, if a tracheostomy is performed in a patient on ECMO, a ST has more advantages (in terms of bleeding control) and is the preferred method [30]. However, as the PDT becomes common place, the scope of the contraindications will gradually decrease. The application of the PDT in patients on ECMO can be a relatively safe procedure if performed by experienced operators, and the critical care team provides adequate management of coagulation and the extracorporeal circuit [26]. Differences exist depending on the type of ECMO used. In this current study there were a higher number of patients on VA ECMO compared with previous reports. Nevertheless, there is a similarity that bleeding complications were overcome by using the PDT in patients on ECMO.
This study has some limitations. The retrospective design may induce a potential bias which may have affected the interpretation of the results. In addition, due to various circumstances of the patients, the application of inclusion criteria may be unclear. In particular, there was a possibility that the criteria for the decision to implement the PDT may be inconsistent in ECMO patients. This was also a limitation of research due to retrospective study design. Furthermore, as a result of incomplete documentation, several less significant complications, such as local stoma infections or minor bleeding, may have been omitted or underestimated. Incomplete documentation made it difficult to retrospectively analyze the effectiveness of early rehabilitation which was mentioned as an advantage of an early tracheostomy, including the functional status of the patients. Besides, the complications associated with coagulation are difficult to conclude within this study. However, it is highly likely that all severe complications were reported because of the clinical importance and were, therefore, identified in the retrospective analysis. Finally, it is not possible to generalize these results because the procedures were performed in a tertiary center with extensive experience in both extracorporeal lung support and applying the PDT.
Conclusion
The PDT procedure may be performed in some patients on ECMO. Anticoagulation during the procedure does not appear to be associated with bleeding complications, although potential bleeding complications from anticoagulant should be considered. ICU staff can perform PDT more actively in patients with coagulation. Further multi-center studies are required to provide clinical evidence regarding the use of PDT in patients with coagulopathy on ECMO.
Notes
Author Contributions
Conceptualization: SHP. Data curation: HSK. Formal analysis: THH. Methodology: THH, SHP. Project administration: THH. Visualization: THH, SHP. Writing - original draft: THH. Writing - review & editing: THH, HWK, SHP.
Conflicts of Interest
No potential conflict of interest relevant to this article was reported.
Ethical Statement
The ethics committees of the Hallym University Institutional Review Board approved this study (approval no.: HALLYM 2020-04-010-002), and the requirement for informed consent was waived due to the retrospective design.