Introduction
In many countries, established trauma care systems use the ŌĆ£Hub-and-SpokesŌĆØ model of care [1ŌĆō3] consisting of a bypass protocol that results in the direct transport of severely injured patients to major trauma centers (MTCs) where there are trauma surgeons and other organ specialists [3].
In the US, the American College of Surgeons Committee on Trauma set the criteria for hospitals to gain trauma center status whereby function and education is assessed, and certification is based on strict criteria [4]. Level III trauma centers function as secondary acute care hospitals (SACHs) in rural areas. The surgeon in charge of trauma treatment has the skills and knowledge necessary for resuscitation, stabilization, and transfer of patients, and maintains an adequate level of treatment supported by regular re-education.
The current trauma emergency medical care system in Japan was established in the mid-1970s and is stratified into primary, secondary, and tertiary hospitals [5,6]. However, there is no system in place to assure its quality, and the requirements and training systems for staff vary widely according to the conditions at each hospital. Furthermore, the number of trauma surgeries has decreased recently; this is in part due to a reduced number of traffic accidents [7], and improvements in interventional radiology. Because of these factors, it has become difficult to provide radical treatment for patients with severe trauma in regional SACHs. However, a comprehensive trauma treatment system for trunk injuries (including transfer to MTCs) has not yet been established, and its introduction is urgently needed.
To address these concerns, there is a need to establish a ŌĆ£Hub-and-SpokesŌĆØ type consolidation system of trauma care. To this end, it is necessary to clarify the trauma care skills that general surgeons working in SACHs, which can be referred to as the ŌĆ£Spoke To this end it is necessary to clarify the trauma care skills that general surgeons working in SACHs, which can be referred to as the ŌĆ£SpokeŌĆØ, should possess to transport severe trauma patients to the MCTs, as well as to train them to be able to perform these skills. The present study was conducted to evaluate and reach a consensus regarding the essential trauma care skills required for general surgeons by conducting expert interviews and a Delphi survey.
Materials and Methods
1. Design
The study methodology comprised research team discussions, expert panel interviews, and Delphi surveys distributed for completion among trauma specialists. An initial list of acute care surgical tasks was created by the research team based on a literature review of previous reports and studies that investigated training in trauma care. This list was emailed, for review and modification, to a panel of six trauma experts (acute care surgeons). A Delphi survey was conducted to establish a consensus based on feedback from trauma specialists.
2. Compilation and review of a list of trauma care skills
A total of 31 items regarding trauma care skills undertaken by general surgeons were compiled through research team discussions including a researcher, surgical educator, and acute care surgeon. In this study, the term ŌĆ£general surgeonŌĆØ included surgeons who practice digestive, cardiovascular, or thoracic surgery. Six experts certified as acute care surgeons by the Japanese Association for Acute Medicine were chosen for the experts to be interviewed. The compiled list of 31 items was sent to these experts via e-mail, and they provided feedback on whether each trauma care skill would be primarily required by general surgeons. This resulted in 33 items being included in the Delphi consensus survey (Table 1).
3. Selection of the Delphi panel
To constitute the Delphi survey panel, invitations were emailed to all 117 councilors of the Japanese Society for Acute Care Surgery (JSACS) with a request to participate in the Delphi consensus survey.
4. Survey process
The Delphi consensus survey was conducted using web-based software (Google Forms). All invited specialists completed the survey rounds.
In the 1st round, participants were presented with a predefined list of 33 items and asked to rate how strongly they agreed or disagreed [using a 5-point Likert scale (1 Strongly disagree, 2 Disagree, 3 Undecided, 4 Agree, and 5 Strongly agree)] with the necessity of each procedure. Moreover, the participants could provide comments/revisions to each item, and add additional relevant trauma care skills which they thought a general surgeon should possess. All survey participants were asked to respond within five weeks, and reminder letters were sent to non-responders approximately two weeks before the deadline.
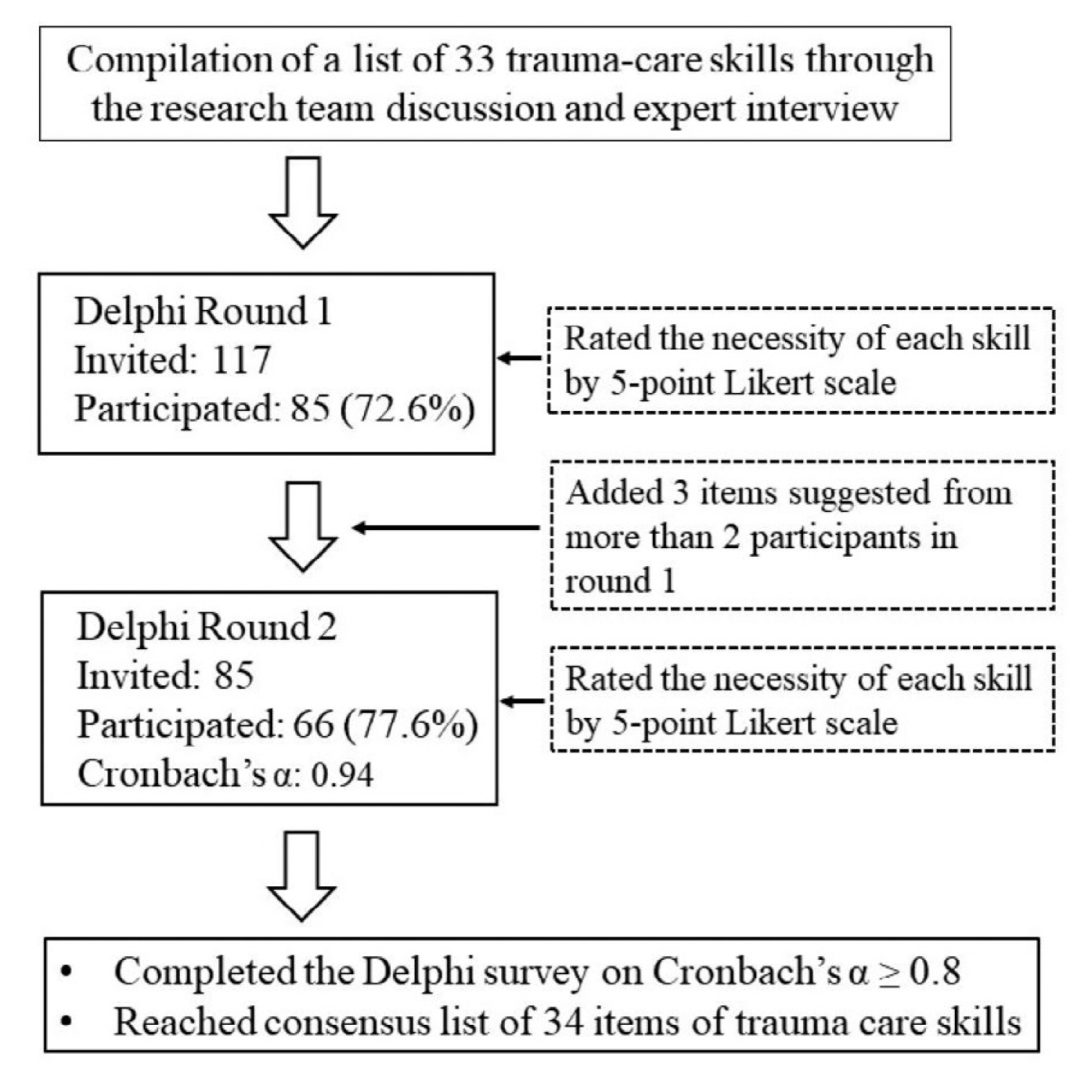
In the 2nd round, participants (1st -round responders) were asked to rate the same 33-item list again, after the results of the 1st round (graphs of group ratings for each item) were shared. Furthermore, these participants were asked to rate new skills that had been suggested for inclusion by more than two participants during the 1st round (Figure 1).
5. Statistical analysis
The mean and 95% confidence intervals were calculated for all procedures. CronbachŌĆÖs ╬▒ was calculated for internal consistency among the responses from specialists. JMP Pro Version 13.1 (SAS Institute Inc., NC, USA) was used for statistical analysis.
6. Consensus decision
It was determined that the Delphi survey would need to be conducted in at least two rounds to reflect accurate results and facilitate reassessment of participant answers (from the 1st round) in a 2nd round of the survey. Consensus was predefined as CronbachŌĆÖs ╬▒ Ōēź 0.8, which has previously been reported as being representative of an acceptable measure of internal reliability [8,9], and the items were retained when they were rated 4 or 5 by Ōēź 80% members of the Delphi survey panel.
7. Ethical considerations
The study protocol was reviewed and approved by the Institutional Review Board of the Faculty of Medicine, Hokkaido University (IRB approval no.: 2017-95). All participants responded to the Delphi consensus survey anonymously to the researcher, and their personal information was protected during data collection and analysis.
Results
1. First round Delphi survey
There were 117 specialists initially contacted, of whom 85 participated in the 1st round of the Delphi survey (response rate: 72.6%). Table 2 shows participant characteristics. In this round, two or more respondents suggested the inclusion of three additional items, ŌĆ£diaphragm repair,ŌĆØ ŌĆ£ostomy,ŌĆØ and ŌĆ£temporary abdominal closure,ŌĆØ to the list.
2. Second round Delphi survey
In the 2nd round of the survey, the 85 specialists who responded in the 1st round were contacted, and 66 participated and rated the skill items in the revised list (response rate: 77.6%). The consensus achieved after two rounds of the survey was reliable (CronbachŌĆÖs ╬▒ score of 0.94), and there were 34 items regarding trauma care skills retained that had responses rated 4 or 5 by Ōēź 80% participants (Table 3).
Discussion
A consensus-based list of trauma care procedural skills required for general surgeons was developed by using interviews with experts and a Delphi survey which returned a high response rate and showed internal consistency. Following expert approval, ŌĆ£tracheal intubation,ŌĆØ ŌĆ£intraosseous infusion,ŌĆØ ŌĆ£focused assessment with sonography for trauma (FAST),ŌĆØ and ŌĆ£non-invasive external pelvic compressionŌĆØ were included in the required trauma care skills for general surgeons. Based on the recommendations from the 1st round of the Delphi survey, ŌĆ£diaphragm repair,ŌĆØ ŌĆ£ostomy,ŌĆØ and ŌĆ£temporary abdominal closureŌĆØ were included in the final list. Since abdominal trauma surgery often involves cases of open abdominal non-closure, the addition of ŌĆ£temporary abdominal closureŌĆØ was considered to be reasonable. Finally, the included 34 items were classified into the following four groups: basic, thoracic, abdominal and pelvic, and vascular skills.
Basic skills (NoŌĆÖs. 1ŌĆō6; Table 3) are included in the Japan Advanced Trauma Evaluation and Care (JATEC) simulation training programs [10], which is the original Japanese trauma training course that was developed in 2002 to inculcate basic process knowledge and skills in trauma care. The JATEC training program was developed with reference to the clinical theory of Advanced Trauma Life Support [11] which is managed by the American College of Surgeons Committee on Trauma. Although basic process skills are required by all physicians involved in trauma care, general surgeons do not always practice these skills, therefore, we have included them in the list.
The purpose of thoracic surgery in trauma cases is to control intrathoracic or pericardial bleeding as well as lung air leaks, and perform decompression for reducing excessive pericardial or intrathoracic pressure [12,13]. ŌĆ£Pericardiostomy,ŌĆØ ŌĆ£heart injury repair,ŌĆØ ŌĆ£pulmonary hilum clamp,ŌĆØ ŌĆ£pulmonary injury repair,ŌĆØ ŌĆ£open cardiac massage,ŌĆØ and ŌĆ£open aorta cross-clampingŌĆØ are essential skills to fulfill the aims mentioned above and are generically called ŌĆ£resuscitative thoracotomy (RT)ŌĆØ [14,15]. It seemed reasonable for these skills to be retained in the list. However, ŌĆ£median sternotomyŌĆØ and ŌĆ£clamshell thoracotomyŌĆØ were rated 4 or 5 by < 80% participants in both rounds of the Delphi consensus survey and therefore were considered ŌĆ£rejected skills.ŌĆØ
In the clinical management strategy for abdominal trauma, it is important to control hemorrhagic shock caused by acute bleeding, and peritonitis secondary to digestive tract injuries. Intraperitoneal bleeding is detected using ŌĆ£FAST;ŌĆØ moreover, a ŌĆ£crash laparotomyŌĆØ is required in patients with a positive FAST who are in a state of shock refractory to intravenous infusion. Therefore, ŌĆ£FASTŌĆØ and ŌĆ£crash laparotomyŌĆØ were considered to be essential skills for treatment of patients with abdominal trauma. Moreover, ŌĆ£five-point gauze packingŌĆØ to control abdominal bleeding and ŌĆ£peri-hepatic gauze packingŌĆØ to control hepatic bleeding are important skills in damage control surgery (DCS). ŌĆ£Peri-hepatic gauze packingŌĆØ is an effective technique for severe liver injury [16]; however, it requires adequate training because, if incorrectly performed, it may cause inadequate hemostasis or complications such as edema of the intestinal tract or venous embolism [17]. Furthermore, ŌĆ£temporary abdominal closureŌĆØ is an essential skill following surgery. In the case of DCS for massive intestinal tract injury, only hemostasis and resection should be undertaken; intestinal anastomosis should be delayed until reoperation 24ŌĆō48 hours later [18]. Therefore, ŌĆ£intestinal injury repairŌĆØ and ŌĆ£bowel resectionŌĆØ were considered important skills for DCS. In case of DCS for colonic injury, ŌĆ£ostomyŌĆØ was not mandatory. Some prospective studies reported that the rate of anastomotic leak for colonic anastomoses was 2.5%, which is acceptable [19,20]. Another study recommended the construction of an artificial anus in patients with severe complications [21]. ŌĆ£OstomyŌĆØ was necessary in case of extraperitoneal rectal injury that could not be sutured [22,23]; therefore, this skill was included.
The ŌĆ£resuscitative endovascular balloon occlusion of the aorta (REBOA)ŌĆØ technique has recently emerged as an alternative method of RT with aortic cross-clamping for non-compressible torso hemorrhage (NCTH). Some studies have compared REBOA and RT. Abe et al [24], and DuBose et al [25] reported that the in-hospital mortality of patients who received REBOA or RT for NCTH did not differ significantly. Conversely, Aso et al [26] reported that the REBOA group had lower mortality and fewer severe chest complications than the RT group. Therefore, REBOA may be another choice for NCTH among general surgeons.
In the US, medical residents are required to undergo a 5-year surgical training program certified by the Accreditation Council for Graduate Medical Education to be board-certified general surgeons [27], and registration of surgical and nonsurgical cases is required for trauma surgery. The American College of Surgeons (ACS)/Association of Program Directors in Surgery surgical resident skills curriculum was developed jointly and includes 16 basic surgical skills, 15 advanced skills, and 10 team-based skills [28]. The list developed in this survey is mostly consistent with this curriculum and partially includes skills in advanced trauma training courses such as Advanced Trauma Operative Management [29] which is provided by the ACS fellowship programs (Table 4). Therefore, our list orders the trauma skill levels of American surgical residents who are part of the ACS fellowship program.
Since trauma training based on the Japanese surgical specialist program includes points from off-the-job training, the required points can be obtained even if there are not enough clinical cases in trauma surgery. The off-the-job training includes specific simulation training programs such as JATEC, Advanced Trauma Operative Management and advanced surgical skills for exposure in trauma [30], as well as trauma workshops sponsored at conferences. Table 4 shows a comparison between the skills for which consensus was obtained in this Delphi survey, and the skills included in each course program. We believe that program development, based on these consensus-based skills, will contribute to the construction of an optimal training system that can supplement procedures that general surgeons cannot learn in the existing courses.
There is a limitation to this study. Since some councilors of the JSACS participating in this survey may not be directly involved in trauma care, there is a possibility that not all participants accurately selected the trauma care skills currently required in clinical cases.
Conclusion
This study determined the trauma care skills required by general surgeons at regional hospitals. This was achieved using a Delphi consensus survey with respondents who were specialists in trauma surgery. These findings facilitate an ŌĆ£essential need assessmentŌĆØ to develop a novel trauma-training program that is optimized for general surgeons. Future research should investigate the proficiency of general surgeons in the primary trauma care skills identified in this study.