외상성 늑골 골절로 유발된 타코츠보 증후군
Takotsubo Syndrome Resulting from Traumatic Multiple Rib Fractures
Article information
Abstract
Takotsubo syndrome, also known as stress-induced cardiomyopathy, is a transient cardiac syndrome that mimics acutecoronary syndrome. This condition should be suspected if the patient presents with chest pain after intense emotional stress, accompanied by an abnormal electrocardiogram, elevated levels of myocardial enzymes, and left ventricular apical akinesia on echocardiography. Coronary angiography should be performed for prompt differentiation from ischemic heart disease. A 77-year-old female presented with traumatic multiple fractures of the left sixth and seventh ribs resulting from a violent strike. Clinical findings of physical examination, laboratory tests, electrocardiogram, and coronary angiography provided the diagnosis of Takotsubo syndrome. We performed conservative management including pain control, and the patient was uneventfully discharged seven days after admission.
서론
타코츠보 증후군(Takotsubo syndrome)은 심초음파 검사상 좌심실심첨부 벽의 비정상 소견을 보이는 심근병증으로, 일반적으로는 극심한 심리적 스트레스로 인한 심근병증(stress-induced cardiomyopathy)으로도 일컫는다[1]. 증상 및 검사소견이 급성심근경색증과 유사하기 때문에 관상동맥조영술로 관상동맥에 뚜렷한 이상 병변이 없음을 확인하기 전에는 감별이 어렵다. 타코츠보 증후군으로 인한 원내 사망률은 10% 미만이고 적절한 치료를 할 경우 완전한 회복을 기대할 수 있기 때문에 정확한 감별진단이 중요하다. 저자들은 외상으로 인해 발생한 타코츠보 증후군의 증례를 보고하고자 한다.
증례
특이 과거력 없는 77세 여자 환자가 타인으로부터 좌측 흉부를 주먹으로 가격당하는 폭행으로 발생한 흉통으로 응급실에 내원하였다. 흉부전산화단층촬영 결과 미세한 다발성 늑골 골절(좌측, 6번∼9번)이 발견되었고, 외상으로 인한 혈흉, 기흉 또는 복부장기 손상은 동반되지 않았다. 초기 활력징후는 혈압 94/65 mmHg, 호흡수 25회/분, 체온 36.5°C였으며, 좌측 흉부 전벽부위의 통증과 어지러움, 위약감 등을 호소하였다. 흉통은 진통제를 투여 받고 안정한 이후로 완화되었으나 움직이거나 기침할 때 악화되었고 전신 위약감은 지속되었다. 좌측 다발성 늑골 골절 진단으로 입원치료 계획 중 심장효소수치검사상 troponin-T 0.763 ng/ml (정상범위 ≤0.014), creatine kinase (CK)-MB 16.61 ng/ml (정상범위 0∼5.0)로 높게 측정되었고, 심전도상 전측벽 허혈(antero- lateral myocardial ischemia)이 의심되는 소견을 보여(Fig. 1A) 심초음파를 시행하였다. 심초음파 결과 심장 전측부 및 심첨부에 심근운동 저하증이 발견되었고(Fig. 2), 급성관상동맥증후군(acute coronary syndrome)을 감별하기 위해 관상동맥조영술을 시행하였다(Fig. 3). 검사 결과상 모든 관상동맥 분지는 정상 소견을 보여 타코츠보 증후군으로 진단할 수 있었다.
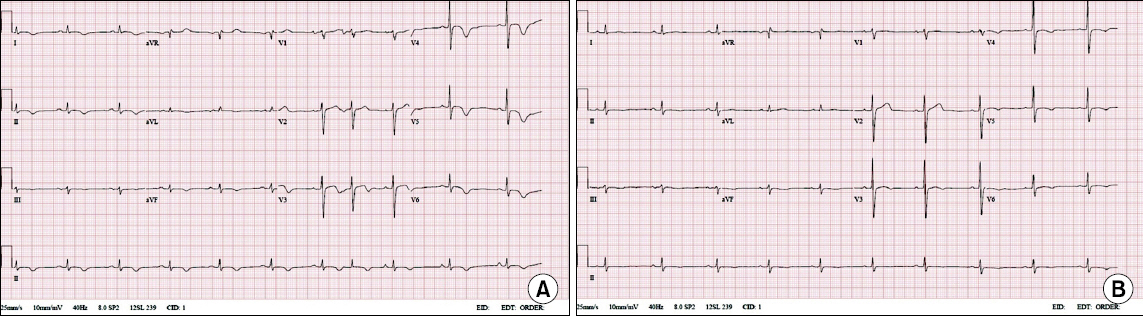
Serial changes in electrocardiograms. The electrocardiogram on admission demonstrates ST-segment elevation in anterior leads, T-wave inversion in inferior leads, and sinus arrhythmia (A). Four days after admission, abnormal findings were converted to nearly normal findings (B).

Echocardiographic findings of Takotsubo syndrome. Transthoracic echocardiography reveals apical ballooning (arrow) of the left ventricle. The apical three chamber view shows dilation and akinesia of the apex in diastole (A) and in systole (B).
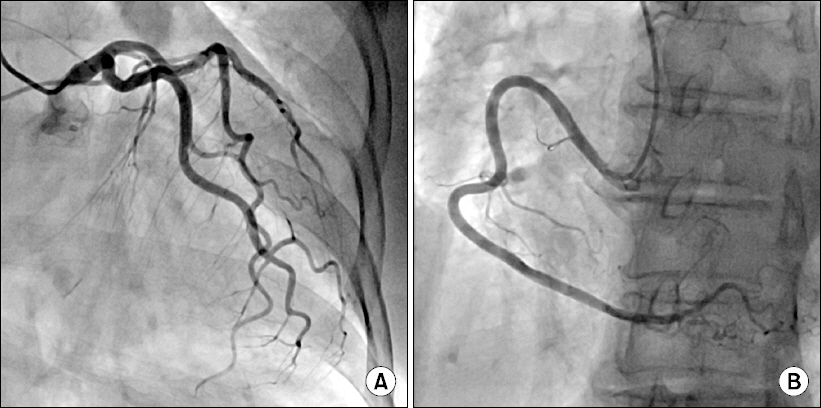
Coronary angiography. Coronary angiography demonstrates no significant stenosis in the left (A) and right (B) coronary arteries.
입원 2일째 심장효소수치검사 결과상 troponin-T 0.111 ng/ml, CK-MB 4.43 ng/ml로 감소하였고, 심장효소수치 및 심전도를 추적 관찰하며 늑골 골절로 인한 흉통 완화 목적으로 진통제를 투약하였다. 입원 후 일주일에 걸쳐 심장효소수치가 정상 범위 내로 회복되었고 심전도상 T-파 역위도 소실되어(Fig. 1B), 경구 진통제를 유지하며 퇴원하였고 6개월 동안 별다른 문제는 관찰되지 않았다.
고찰
타코츠보는 일본어로 문어잡이 항아리를 뜻한다. 타코츠보 증후군에서 보이는 특징적인 심초음파 소견인 좌심실 심첨부 확대(apical ballooning)가 이와 유사한 모양에서 기인하였다. 타코츠보 증후군 환자의 가장 흔한 증상인 흉통은 흉부 외상 환자의 증상과 유사하므로 타코츠보 증후군 진단은 간과될 수 있다. 따라서 흉부 외상 환자에서 급성 좌심실 기능장애가 나타났을 때 타코츠보 증후군은 감별진단에 포함되어야 한다. 본 증례인 경우, 늑골 골절 부위가 심장이 위치한 부위와 일치하기 때문에 응급실 내원 당시부터 심장에서 기인한 통증으로 생각할 수는 없었다. 따라서 환자의 증상을 면밀히 관찰하고 추적 관찰하는 것이 중요하다.
타코츠보 증후군의 원인과 병태생리는 명확히 밝혀지지 않았지만, 심리적 스트레스와 관련된 카테콜아민 격동(catecholamine surge)에 의한 심근병증 발생이 가장 가능성 있는 가설이다[2]. 카테콜아민은 심장에 관여하는 교감신경계를 교란시키고 관상동맥의 미세혈관 연축을 일으켜 심근의 특징적인 수축 양상과 허혈 손상을 초래할 수 있다[3].
Mayo clinic에서 제시한 진단 기준은 다음과 같으며[4], 명백한 스트레스 사건 발생과 함께 모두 만족해야 진단 가능하다. 1) 첨부 병발이 동반되거나 혹은 동반되지 않은 좌심실 중간부의 일과성 운동이상, 2) 폐쇄성 관상동맥 질환 없음, 3) 새롭게 나타난 심전도 이상 소견(ST-분절 상승 또는 T-파 역위) 혹은 심근효소 중 troponin 수치 상승, 4) 크롬친화세포종(pheochromocytoma)이나 심근염의 증거 없음 등이다. 본 증례에서는 극심한 심리적 스트레스 요인은 불분명하나, 흉부 외상으로 인해 나타난 증상들이 위 진단 기준들을 모두 충족하고 있고 자연경과 역시 타코츠보 증후군으로 진단하기에 충분하다고 보인다.
타코츠보 증후군은 급성 심근경색과 유사한 일과성 좌심실 기능장애가 나타나지만, 이와는 달리 타코츠보 증후군 환자의 약 95%가 4∼8주 이내에 완전히 회복하기 때문에 대증적 치료 외에 특정한 치료 지침은 없다[5,6]. 본 증례에서도 진통제를 투여하며 경과 관찰하였고 입원 7일째 호전되어 퇴원이 가능하였다. 초기 발병 이후 4년 이내에 재발할 확률이 11%로 보고되고 있으므로[7], 이 환자의 경우 추후 흉부 외상을 경험하게 된다면 타코츠보 증후군 여부를 확인해야 한다.
결론
흉부 외상으로 인한 흉통을 호소하는 환자에서 심전도 이상 소견과 심근효소 상승을 동반한 경우에는 타코츠보 증후군을 의심해야 하며, 심장초음파에서 심장 전측부 및 심첨부에 심근운동 저하증이 발견되는 경우에는 급성심근경색증과 감별하기 위해 관상동맥조영술을 고려해야 한다.
Conflicts of Interest
No potential conflict of interest relevant to this article was reported.