Successful Simultaneous Endovascular Repair of Traumatic Portal Vein Pseudoaneurysm and Aortic Injury
Article information
Body
A 50-year-old man visited to the trauma center after driver traffic accident. Multiple injuries were found on computed tomography (CT) scan including aortic injury, duodenal perforation, pancreas contusion, and portal vein aneurysm (Fig. 1). Exploratory laparotomy was performed immediately for control of bleeding, primary repair of perforated duodenum, transverse colon and stomach. As soon as the operation was completed, the patient was transferred to the angio-room. The endovascular repair for aorta and portal vein was performed (Fig. 2). The patient was discharged from the hospital 3 months later, without disability and complication. At 1-year follow up CT scan revealed no endoleak and good patency of stent-graft (Fig. 3).
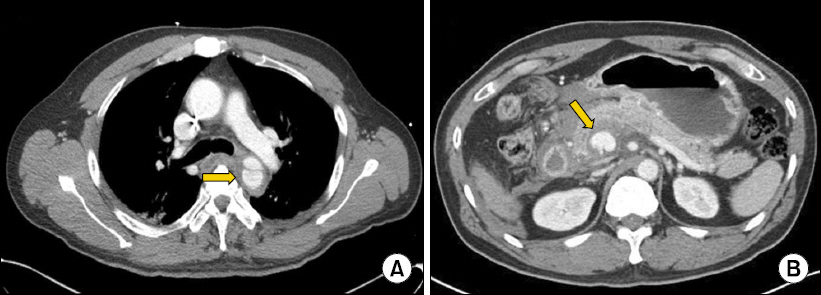
Initial computed tomography (CT) scan. (A) Contrast enhanced CT scan of the chest revealed a 3 cm long pseudoaneurysm at the isthmus of the aorta (arrow) and intramural hematoma in the descending thoracic aorta. (B) Venous phase image of the abdominal CT scan demonstrates a 2 cm portal vein aneurysm (arrow) and hematoma around the pancreas head.

Endovascular repair. (A, B) Transhepatic portography shows a portal vein pseudoaneurysm just proximal to the joining of the superior mesenteric vein (SMV) and splenic vein. (C) Viabahn stent graft (W.L. Gore, Flagstaff, Ariz) in SMV and portal vein.
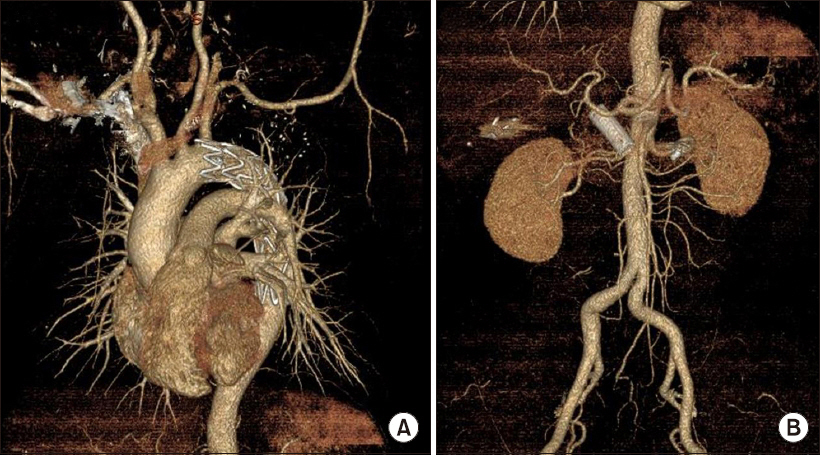
Three-dimensional aorta angiography 1-year postoperative. (A) Transendovascular aortic repair indicated a complete resorption of the traumatic aortic dissection. (B) Stent graft insertion in the portal vein indicated good patency and no endoleak. Embolization of the traumatic pseudoaneurysm of the midcolic artery showed no extravasation or bowel ischemic change
Traumatic aortic injury (TAI) is the second most common cause of death from blunt trauma. Paradigm of TAI treatment has changed from open surgery to endovascular repair because of the benefits of minimal invasiveness and avoidance of full heparinization in multiple trauma patients [1]. Although pseudoaneurysm of the post-traumatic portal vein rarely occurs, surgical mortality is also high because of the difficulty in maintaining hemostasis and the secondary damages associated with enteric and pancreatic injuries [2,3]. Combined angiographic and surgical approaches could provide advantages for exsanguinating patients with multiple injuries and especially for management of major vascular, high-grade liver, or pelvic bleeding [4,5]. We achieved a good result through combined endovascular open surgical treatment in the patient who required the management of damage control resuscitation.
Acknowledgments
This work was supported by clinical research grant from Pusan National University Hospital in 2017.
Conflicts of Interest
No potential conflict of interest relevant to this article was reported.
References
Notes
Conflicts of Interest
No potential conflict of interest relevant to this article was reported.