Multiple Surgical Treatments for Recurrent Retroperitoneal Hemorrhage in a COVID-19 Patient with Respiratory Failure on Extracorporeal Membrane Oxygenation
Article information

Abstract
Extracorporeal membrane oxygenation (ECMO) may be required in patients with corona virus disease-19 (COVID-19) and respiratory failure. Anticoagulation is the standard treatment to prevent complications of ECMO and COVID-19 coagulopathy, however, there is a risk of bleeding. Some patients with retroperitoneal hemorrhage (RPH) have been treated with angiography-embolization. We report on a patient with COVID-19 on ECMO who underwent multiple operations (×5) for recurrent RPH. A 46-year-old man was admitted with COVID-19 pneumonia. ECMO with anticoagulation therapy was initiated. The patient developed RPH, caused by external compression of the inferior vena cava interrupting the ECMO inflow, and surgical hematoma evacuation was performed, with no obvious bleeding focus during the multiple surgeries. Following the patient’s recovery, a follow-up computed tomography scan showed the hematoma had been resolved, but there was a dilemma regarding anticoagulation. Lowering the threshold for surgical treatment, enabled treatment of a patient with serious RPH.
Introduction
Coronavirus disease-19 (COVID-19) became a global pandemic in 2020. The clinical features have been extensively published, ranging from asymptomatic infection to acute respiratory failure, requiring invasive mechanical ventilation (MV) [1]. Acute respiratory distress syndrome (ARDS) develops in 42% of patients who present with COVID-19 pneumonia, and of those patients, 61–81% require intensive care [2].
The application of extracorporeal membrane oxygenation (ECMO) for patients with severe ARDS is a promising modality to correct refractory hypoxia and prevent lung injury caused by prolonged MV. However, ECMO has its own complications, including those which result from the contact between blood and artificial surfaces such as additional inflammatory cascades, bleeding, and thrombosis [3]. Therefore, a significant challenge that arises in these situations is to maintain adequate anticoagulation.
Spontaneous retroperitoneal hematoma (RPH) is potentially fatal [4]. The known risk factors of RPH are anticoagulation therapy and chronic renal failure [5]. COVID-19 is often accompanied by coagulation disorders, and the use of heparin in patients with severe COVID-19 during ECMO treatment accelerates the risk of bleeding [6]. Several cases of RPH have been reported among COVID-19 patients on ECMO [6–8], although most patients recover following blood transfusion and radiological intervention.
We report a case of severe RPH during ECMO in a COVID-19 patient who had multiple surgical treatments. This is the 1st case report, to our knowledge, of surgical treatment for RPH in a patient with COVID-19 on ECMO.
Case Report
This study was approved by the Institutional Review Board of Jeju National University Medical Center (IRB no.: JEJUNUH 2021-12-020). Written informed consent was obtained from the patient for the publication.
A 46-year-old man visited the Emergency Department with a fever and shortness of breath. The patient’s oxygen saturation level was significantly low (60%) indicating the need for supplemental oxygen. A chest X-ray revealed diffuse infiltrates in both lungs (Figure 1). The patient was initially diagnosed with COVID-19 associated ARDS and was admitted to an isolated intensive care unit. As symptoms worsened, full ventilation support was provided. Despite optimal ventilation support, the patient was not able to maintain sufficient oxygen saturation. Therefore, on Hospital Day (HD) 2 the ECMO was applied. Intravenous heparin was administered to maintain an activated partial thromboplastin time of 50–80 seconds.
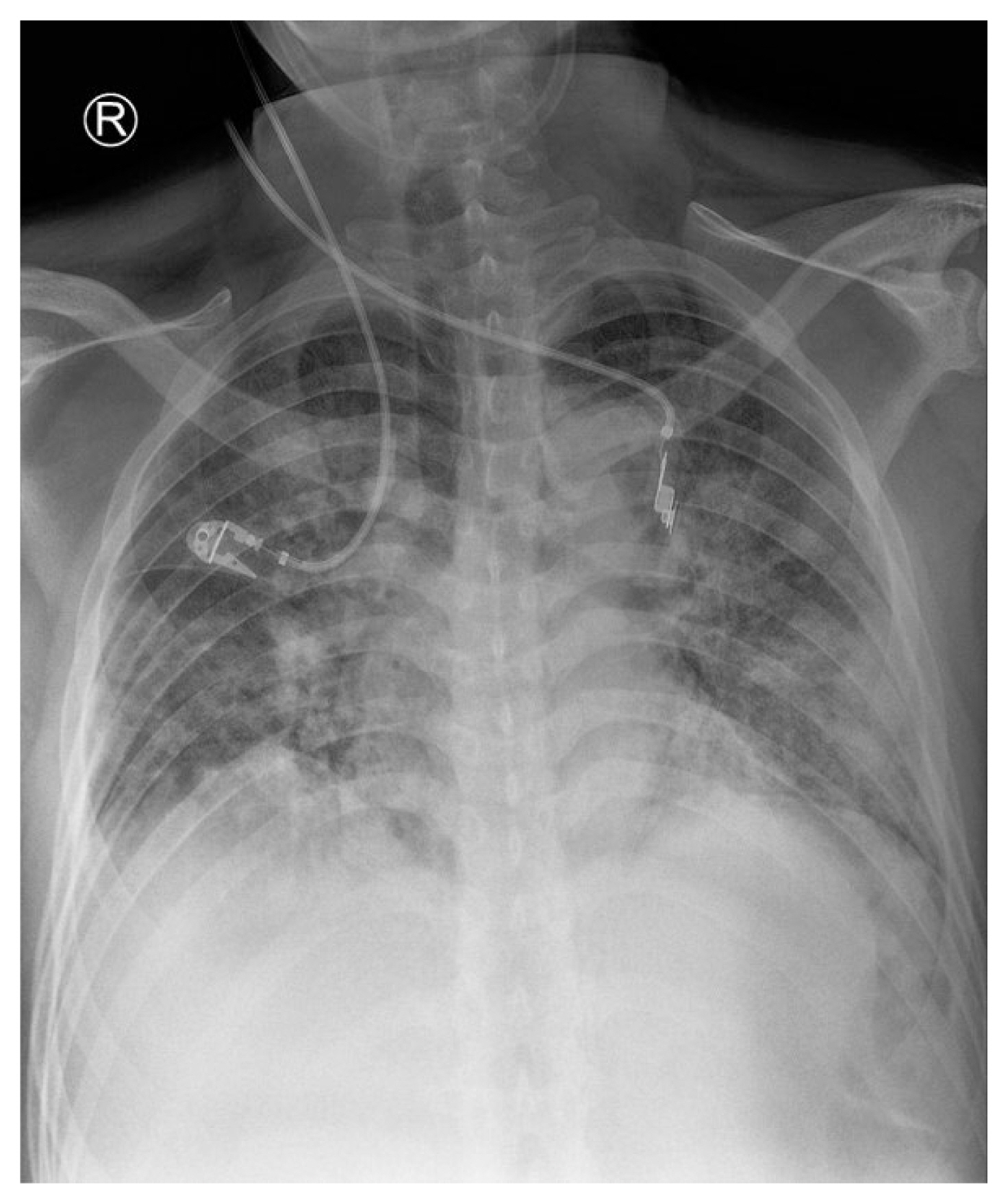
Chest X-ray showed diffuse infiltration of both lungs.
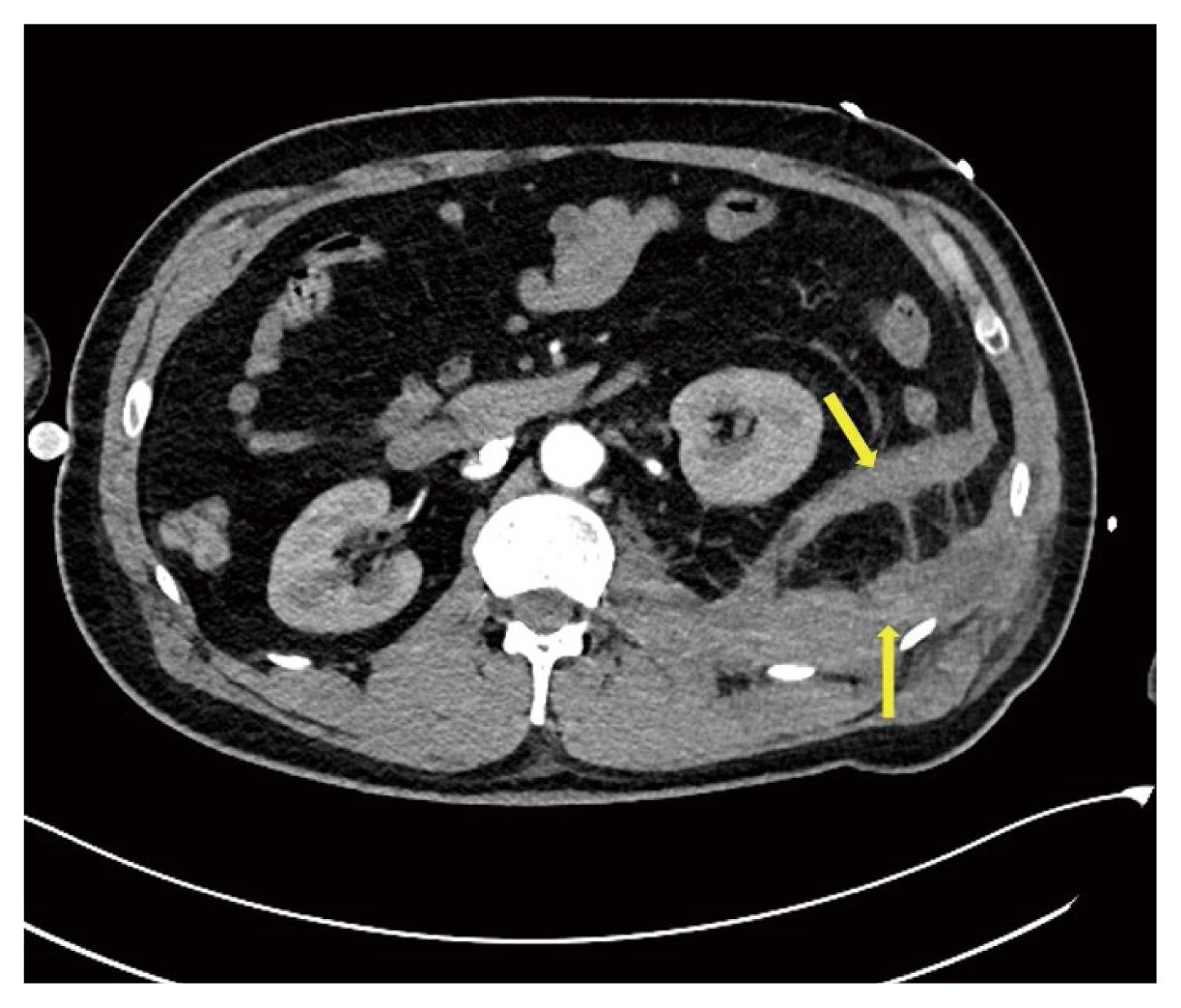
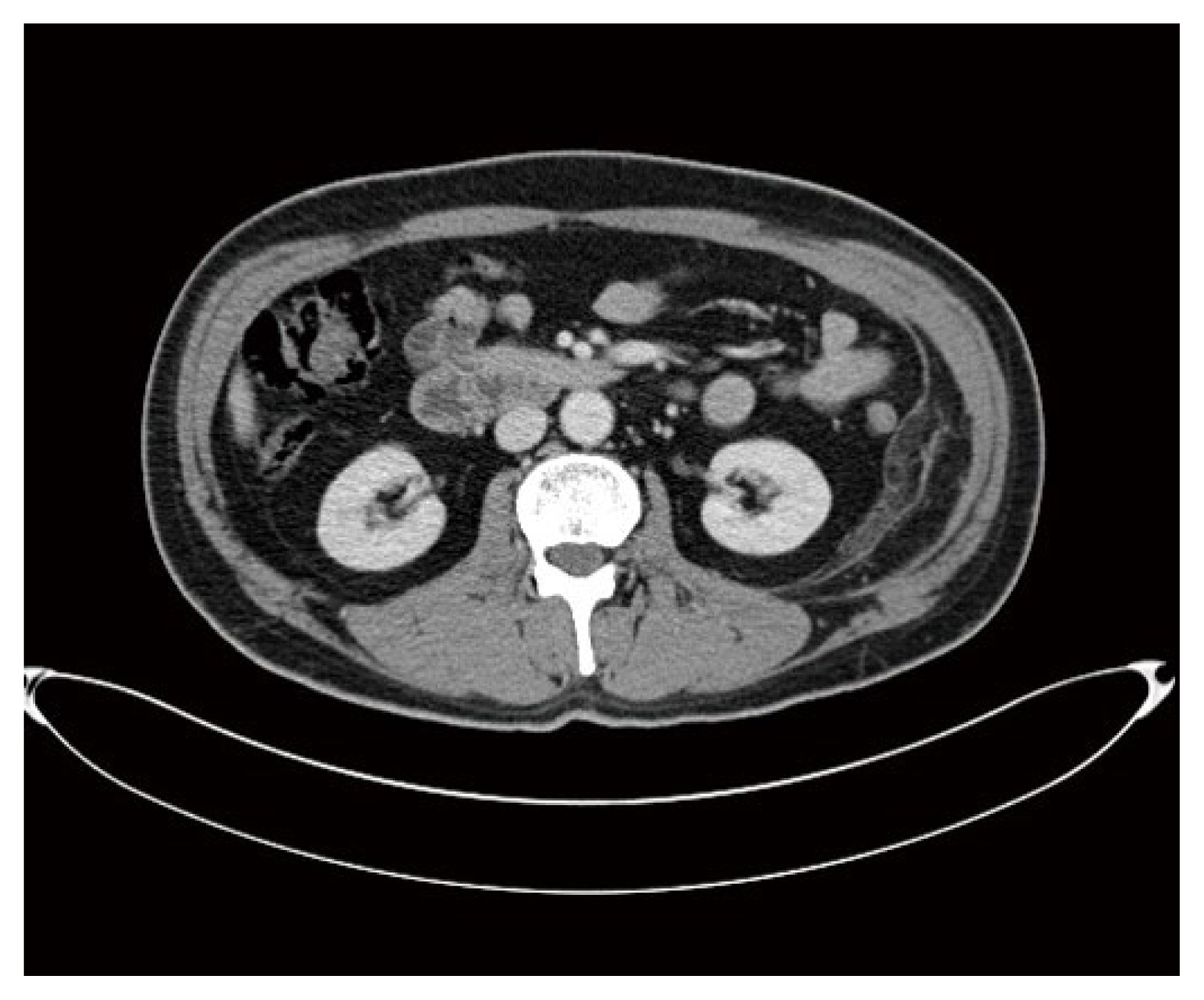
A follow-up computed tomography (CT) chest scan was performed on HD 9, and a retroperitoneal hemorrhage was incidentally uncovered (Figure 2). Heparin was discontinued immediately, and the patient was given a blood transfusion. On HD 13, the abdominal CT scan was repeated, and results showed external compression of the inferior vena cava (IVC) and enlargement of the RPH, which had interfered with the ECMO and significantly reduced inflow (Figure 3). Initially, an angiography with embolization had been considered, however, the hematoma was growing rapidly, and without an observable bleeding focus, direct surgical intervention was performed.
Incidental finding of retroperitoneal hematoma from follow-up
CT scan of the chest on HD 9.
CT = computed tomography; HD = Hospital Day.

Abdominal CT scan on HD 13. (A) multifocal active arterial bleedings (red arrow) in the left retroperitoneum; (B)
IVC had entirely collapsed (yellow arrow).
CT = computed tomography; HD = Hospital Day; IVC = inferior vena cava.
A hockey stick incision was made in the left abdomen to open the retroperitoneal space, and the massive hematoma was pushed out. As the hematoma was evacuated, the ECMO flow recovered to 2.5 L/min from less than 0.7 L/min, and ECMO flow was properly maintained. We tried to find the bleeding focus but only observed diffuse oozing without a prominent bleeding focus in the operative field (Figure 4). Gauze packing was conducted carefully whilst monitoring the ECMO flow to control diffuse oozing and to prevent compression of the IVC by the packed gauze. The fascial layer was approximated, and the skin was closed using a skin stapler. A wound vacuum device (Curavac, CGBIO, Seongnam, South Korea) was employed with minimal negative pressure. On HD 17, a 2nd operation was performed because the patient’s condition was similar to that which led to the 1st surgery, so the same procedure was repeated.
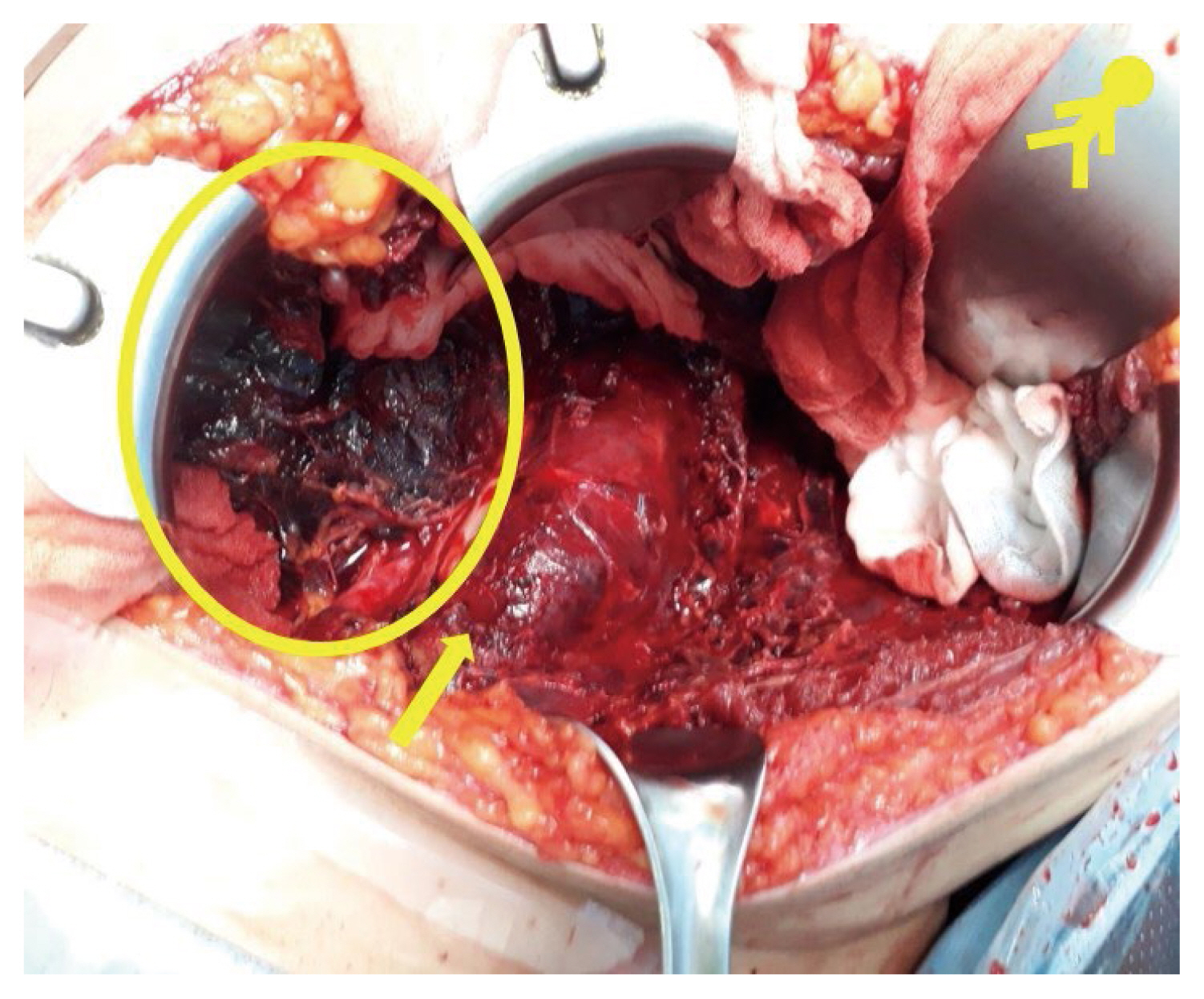
The 2nd surgery after the hematoma was evacuated (HD 17). There was no obvious bleeding focus. Diffuse oozing in the tissue continued. The yellow circle shows the remaining hematoma and the yellow arrow shows a psoas muscle with a muscular hematoma.
HD = Hospital Day.
Following the 2nd surgery on HD 19, angiography and embolization of the left deep circumflex iliac artery were performed, but bleeding persisted, which indicated that the patient had to undergo surgeries for serial bleeding control (Figure 5). On HD 23 and HD 25, hematoma evacuation with gauze packing was repeated. Meanwhile, ECMO was continued until HD 26, after which, with improving lung function, the patient was weaned off ECMO. During the 5th surgery, the oozing was significantly reduced, so we could perform a definite surgery with placement of a Jackson-Pratt drain. Subsequently, there was no further bleeding as ascertained by a follow-up CT scan on HD 39 (Figure 6). From the 5th surgery, hemoglobin levels were becoming stable and there was no need for further transfusions (Figure 7).

Angiography on HD 19. (A) suspicion of bleeding (yellow circle) in the territory of the left deep circumflex iliac artery (yellow arrow); (B) no more bleeding after embolization.
HD = Hospital Day.

Follow-up CT scan after the 5th surgery on HD 39 showed a markedly decreased extent of left retroperitoneal hematoma.
CT = computed tomography; HD = Hospital Day.
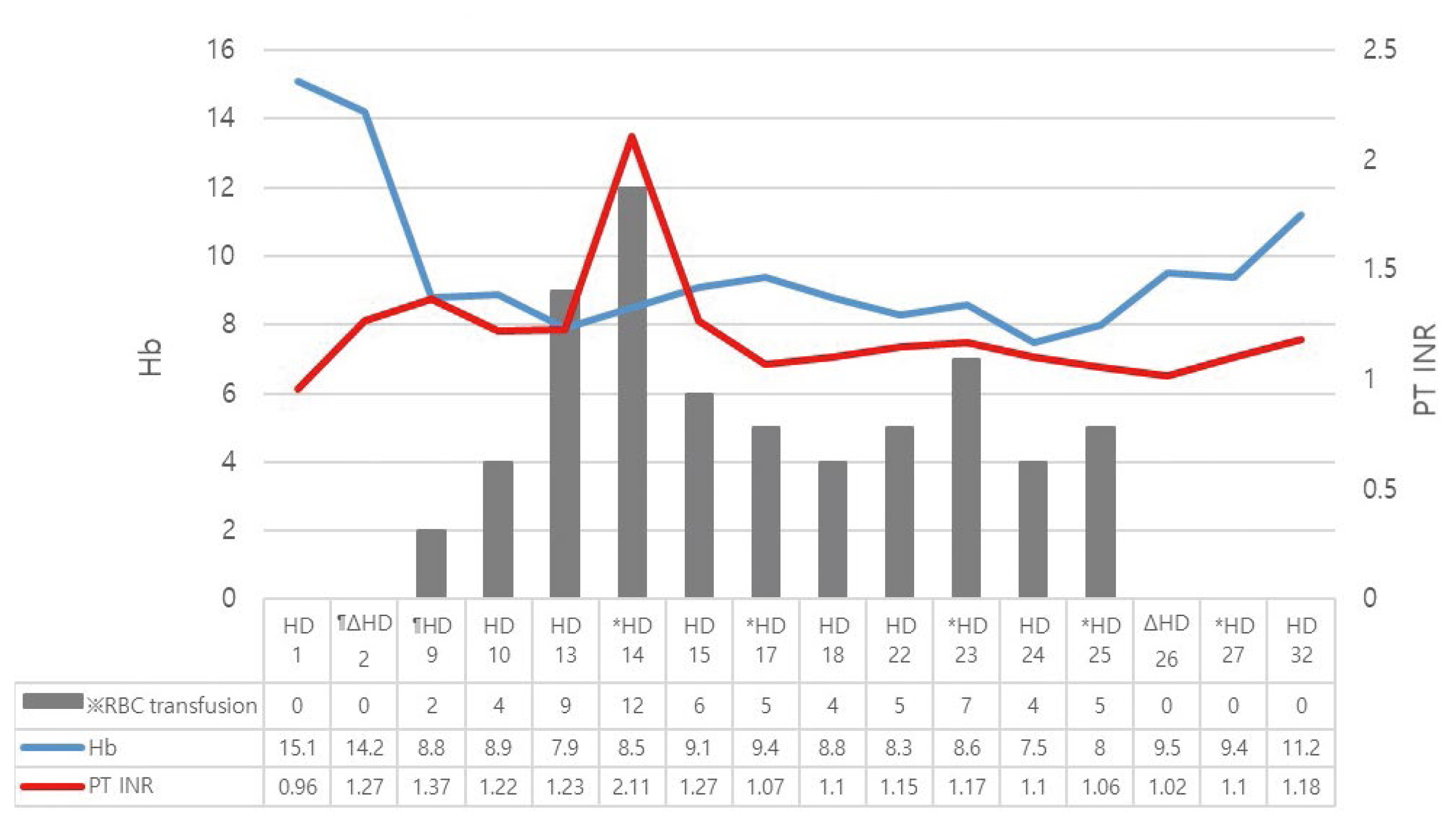
Hb, PT INR and RBC transfusion. The level of hemoglobin change in the patient. Systemic anticoagulation was stopped immediately as the retroperitoneal hematoma was detected on HD 9.
* Operation day (5 surgeries performed in total).
¶ Systemic anticoagulation was provided from HD 2 to HD 9
Δ ECMO was applied from HD 2 to HD 26.
ECMO = extracorporeal membrane oxygenation; HD = Hospital Day
A follow-up CT scan in the clinic on HD 63, showed the hematoma had nearly disappeared and the patient was discharged (Figure 8).
Follow-up CT scan 2 months after the last surgery showed that the retroperitoneal hematoma had nearly disappeared.
CT = computed tomography.
Discussion
Severe COVID-19 can lead to viral pneumonia and ARDS. Severely ill patients with COVID-19 can frequently be observed with coagulopathy and disseminated intravascular coagulation-like massive intravascular clot formation. The clinical presentation of coagulopathy is primarily organ dysfunction, while hemorrhagic events are less frequent. Anticoagulant therapy has been reported to achieve better outcomes in patients with severe COVID-19 when there are signs of coagulopathy requiring MV [9–13]. Hence, standard anticoagulant therapy is strongly recommended [9]. ECMO can be used to treat patients with severe ARDS [1], but, possible complications must be considered, especially thrombosis [3]. Considering this, anticoagulant therapy was started. With the accumulation of data for severely ill patients with COVID-19, case reports of bleeding complications from the use of anticoagulant are being reported more frequently. Typically, these reports advise caution regarding the risk of bleeding [6–8,14–16], but despite the acknowledged risk of bleeding, the use of an anticoagulant for the stable use of ECMO is inevitable.
Recently, RPHs have been reported in patients with COVID-19 where an anticoagulant has been used. Most patients were treated using embolization where there was a clear bleeding focus [6–8,14–16]. In this study, no obvious bleeding focus was observed on the CT scan, and the ECMO flow was not properly maintained due to external compression by a huge RPH. Therefore, surgical intervention was necessary.
During the surgery, a definite bleeding focus was not observed (except for diffuse oozing from the surrounding tissues). The compression of the IVC by the hematoma was alleviated by hematoma evacuation and gauze packing to prevent further bleeding.
The use of systemic procoagulants was also considered, but thrombus-induced-malfunction of ECMO in the situation has been reported to result in the patient still being very dependent on ECMO [17], and the end organ damage from microthrombus and fibrin deposition caused by systemic pro-coagulation was of concern [18,19].
Between the 2nd and 3rd surgery, an angiography and left deep circumflex iliac artery embolization were performed, but this alone was not sufficient to explain the previous bleeding and prevent further hemorrhage. Oozing in the tissue had significantly reduced which was confirmed in the patient during the 5th surgery.
Bleeding control by embolization is an effective method to use when a clear bleeding focus can be localized. However, our patient, who had systemic coagulopathy caused by COVID-19 with intravenous anticoagulation for ECMO use, had a strong tendency towards diffuse tissue oozing without definite bleeding focus. For this specific case, bleeding control surgery with the correction of coagulopathy by blood transfusion must be considered early.
Notes
Author Contributions
Conceptualization: WBC. Methodology: JRY and WBC. Formal investigation: YMP and JRY. Data analysis: YMP and JRY. Writing original draft: YMP and WBC. Writing - review and editing: JRY and WBC.
Conflict of Interest
The authors declare that they have no competing interests.
Funding
None.
Ethical Statement
This study was approved by the Institutional Review Board of Jeju National University Medical Center (IRB no.: JEJUNUH 2021-12-020). Written informed consent was obtained from the patient for the publication.
Data Availability
All relevant data are included in this manuscript.